Meta-analysis and network meta-analysis of time-to-event outcomes with non-proportional hazards: a Bayesian time-varying hazard ratio approach
Pith reviewed 2026-05-21 06:01 UTC · model grok-4.3
The pith
When the proportional hazards assumption fails, a bivariate Bayesian meta-analysis of treatment and treatment-log(time) interaction coefficients from per-study Cox models produces usable time-varying hazard ratios.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
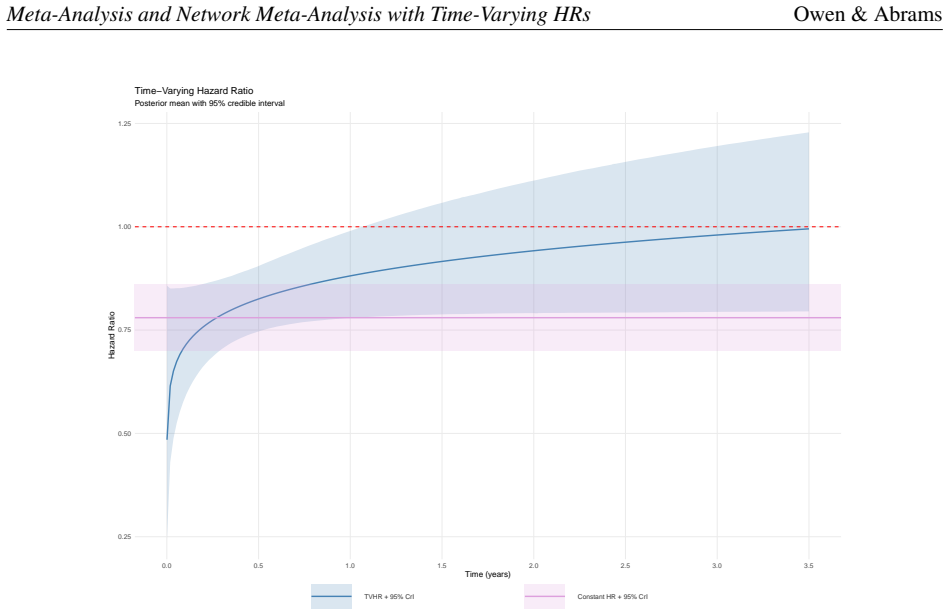
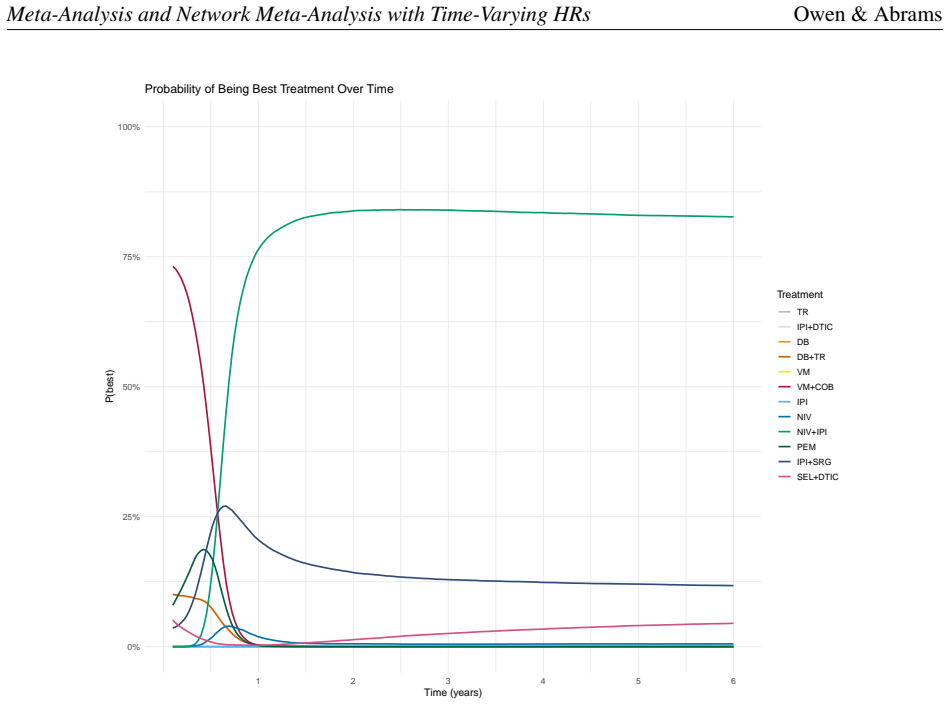
By assuming a treatment-log(time) interaction term within a Cox proportional hazards model for each study and then undertaking a bivariate meta-analysis of the treatment and interaction coefficients, an overall time-varying hazard ratio can be obtained for meta-analysis or network meta-analysis of time-to-event outcomes. In the gastric cancer example the approach produced hazard ratios ranging from 0.83 at 0.5 years to 0.99 at 3.5 years; in the melanoma network the combination immunotherapy showed a hazard ratio improving from 0.37 at one year to 0.24 at five years. The resulting time-varying estimates are presented as intuitive and directly applicable in health technology assessment.
What carries the argument
Bivariate meta-analysis of the treatment coefficient and treatment-log(time) interaction coefficient obtained from per-study Cox models, yielding a time-varying hazard ratio (TVHR).
If this is right
- The obtained time-varying hazard ratios can be read directly at chosen time points for use in economic models and health technology assessment submissions.
- The method applies equally to pairwise meta-analysis and to network meta-analysis while preserving the hazard ratio scale.
- Credible intervals around the time-varying hazard ratio reflect uncertainty arising from both within-study and between-study variation.
- When non-proportional hazards are detected, the approach avoids reliance on a single constant hazard ratio that misrepresents the data.
Where Pith is reading between the lines
- The same bivariate structure could be extended to individual-patient-data meta-analysis to allow study-specific interaction slopes while borrowing strength across trials.
- Similar non-proportionality problems arise in long-term survival extrapolation for cost-effectiveness models; the time-varying hazard ratio supplies a direct way to parameterise waning or strengthening effects.
- Neighbouring methods that use fractional polynomials or restricted cubic splines for the interaction could be compared head-to-head on the same datasets to test robustness of the log(time) choice.
Load-bearing premise
That a treatment-log(time) interaction term within a Cox model for each study sufficiently captures the form of non-proportional hazards present in the included trials.
What would settle it
Re-fitting the same trial data with a more flexible model such as Royston-Parmar splines or time-dependent coefficients and finding that the resulting time profile of hazard ratios differs materially from the log(time)-interaction estimates.
Figures




read the original abstract
Background: Often when undertaking meta-analyses of time-to-event (TTE) outcomes, especially in a Health Technology Assessment context, a hazard ratio (HR) scale is used. However, issues arise when there is evidence of non-proportional hazards in some of the studies included. A number of methods have been advocated, but their use has been limited by either their complexity and/or the ease with which their results can be used in HTA. An alternative approach is to assume a treatment-log(time) interaction within a Cox proportional hazards model for each study, and to then undertake a bivariate meta-analysis of the resulting treatment and interaction coefficients, so that an overall time-varying HR (TVHR) can be obtained. Methods: A TVHR approach was applied to a meta-analysis of chemotherapy compared to Standard of Care for advanced recurrent gastric cancer, and in which Progression-Free Survival (PFS) was an outcome. The approach was also applied to a network meta-analysis (NMA) evaluating overall survival (OS) in advanced BRAF-mutated melanoma. Results: Five trials in the advanced gastric cancer meta-analysis displayed evidence of non-proportional hazards for PFS. Using a TVHR model produced HRs ranging from 0.83 (CrI:0.75-0.91) at 0.5 years to 0.99 (CrI:0.79-1.23) at 3.5 years. Three studies showed evidence of non-proportional hazards in the advanced BRAF-mutated melanoma NMA for OS. Using a TVHR model, nivolumab plus ipilimumab demonstrated consistent superiority from month 7 onwards, with a HR improving from 0.37 (CrI:0.26-0.51) at one year to 0.24 (CrI:0.12-0.45) at five years. Conclusions: A TVHR approach to the meta-analysis or NMA of TTE outcomes when the proportional hazards assumption appears not to hold, produces an intuitive solution which can be readily used in HTA.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes a Bayesian time-varying hazard ratio (TVHR) approach for meta-analysis and network meta-analysis of time-to-event outcomes when the proportional hazards assumption does not hold. It fits a Cox model with a treatment-by-log(time) interaction term to each study, extracts the two coefficients, and feeds them into a bivariate random-effects meta-analysis (or NMA extension) to derive overall time-varying HR trajectories. The method is applied to a meta-analysis of PFS in advanced recurrent gastric cancer (five trials with NPH) and an NMA of OS in advanced BRAF-mutated melanoma (three studies with NPH), producing time-dependent HR estimates presented as suitable for HTA use.
Significance. If the modeling assumptions hold, the approach offers a practical extension of standard Cox and bivariate meta-analysis tools that yields intuitive, time-dependent HRs directly usable in health technology assessment. The two real-data applications demonstrate the method's ability to produce changing HRs (e.g., gastric cancer PFS HR from 0.83 at 0.5 years to 0.99 at 3.5 years; melanoma NMA showing improving superiority for nivolumab plus ipilimumab). Credit is due for grounding the framework in familiar machinery and focusing on HTA applicability rather than purely theoretical derivation.
major comments (2)
- [Methods (TVHR model)] Methods section (TVHR construction): The central claim rests on the treatment-log(time) interaction term within each study's Cox model being a sufficient summary of non-proportional hazards. This parametric choice is load-bearing because the extracted coefficients are then pooled via bivariate meta-analysis; if the true NPH pattern is non-monotonic, involves crossing hazards, or varies qualitatively across studies, the coefficients will be misspecified and the resulting TVHR trajectory will propagate that error. The applications report significant interactions but provide no diagnostic evidence (e.g., Schoenfeld residual plots or comparison to alternative forms) that the log-linear interaction matches the observed data signatures.
- [Results] Results (applications and model reporting): The manuscript reports plausible numerical TVHR results from the two applications yet omits model diagnostics, sensitivity analyses to Bayesian prior choices on the meta-analysis parameters, and direct comparisons against alternative non-PH methods. These omissions are load-bearing for the claim that the TVHR approach produces a robust, readily usable solution for HTA, as the soundness of the pooled estimates cannot be fully assessed without them.
minor comments (1)
- [Abstract and Results] The abstract and results sections would benefit from explicit reporting of MCMC convergence diagnostics or effective sample sizes for the Bayesian bivariate meta-analysis fits.
Simulated Author's Rebuttal
We thank the referee for their constructive and detailed review of our manuscript. We appreciate the emphasis on methodological robustness and have addressed each major comment below. Where revisions are warranted, we have indicated the changes to be made in the next version of the manuscript.
read point-by-point responses
-
Referee: Methods section (TVHR construction): The central claim rests on the treatment-log(time) interaction term within each study's Cox model being a sufficient summary of non-proportional hazards. This parametric choice is load-bearing because the extracted coefficients are then pooled via bivariate meta-analysis; if the true NPH pattern is non-monotonic, involves crossing hazards, or varies qualitatively across studies, the coefficients will be misspecified and the resulting TVHR trajectory will propagate that error. The applications report significant interactions but provide no diagnostic evidence (e.g., Schoenfeld residual plots or comparison to alternative forms) that the log-linear interaction matches the observed data signatures.
Authors: We agree that the treatment-by-log(time) interaction imposes a specific parametric form on the non-proportional hazards and does not capture all possible patterns, such as non-monotonic effects or qualitative differences across studies. This form was selected for its direct interpretability as a time-varying hazard ratio and its compatibility with standard Cox regression and subsequent bivariate meta-analysis. To strengthen the manuscript, we will add Schoenfeld residual plots (or scaled Schoenfeld residuals against log(time)) for each included study in the revised Methods and Results sections to provide diagnostic evidence supporting the interaction term. We will also expand the Discussion to explicitly acknowledge the limitations of this assumption and note that alternative specifications (e.g., time-dependent covariates or spline-based approaches) could be explored in future work when data permit. revision: yes
-
Referee: Results (applications and model reporting): The manuscript reports plausible numerical TVHR results from the two applications yet omits model diagnostics, sensitivity analyses to Bayesian prior choices on the meta-analysis parameters, and direct comparisons against alternative non-PH methods. These omissions are load-bearing for the claim that the TVHR approach produces a robust, readily usable solution for HTA, as the soundness of the pooled estimates cannot be fully assessed without them.
Authors: We acknowledge that additional diagnostics and sensitivity checks would improve transparency and support the claim of robustness for HTA applications. In the revised manuscript we will include: (i) Bayesian model diagnostics such as trace plots, Gelman-Rubin statistics, and effective sample sizes for the meta-analysis parameters; (ii) sensitivity analyses varying the prior distributions on the between-study covariance matrix and mean effects, with results presented in supplementary tables; and (iii) a brief comparison of the TVHR results against at least one alternative non-PH approach (e.g., landmark analysis or restricted mean survival time differences) for the gastric cancer example where individual-patient data are available. These additions will be placed in the Results and Supplementary Materials sections. revision: yes
Circularity Check
No circularity: standard Cox-plus-bivariate-meta framework with no reduction to fitted inputs
full rationale
The paper presents a modeling workflow: fit a Cox model containing a treatment-by-log(time) interaction term separately in each study, extract the two coefficients, and feed them into a bivariate random-effects meta-analysis (or NMA extension) to produce a time-varying HR trajectory. This chain relies on well-established, externally validated statistical components (Cox partial likelihood and standard bivariate meta-analysis) rather than any derivation that equates its output to its inputs by construction. No self-citations are load-bearing, no uniqueness theorems are invoked, and no ansatz is smuggled via prior work. The reported TVHR values are direct consequences of the chosen parametric form applied to the observed data, not a renaming or re-derivation of the same quantities.
Axiom & Free-Parameter Ledger
free parameters (1)
- Bayesian priors on meta-analysis parameters
axioms (1)
- domain assumption A treatment-log(time) interaction within the Cox model captures the non-proportional hazards present in the data
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
assume a treatment-log(time) interaction within a Cox proportional hazards model for each study, and to then undertake a bivariate meta-analysis of the resulting treatment and interaction coefficients
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Shannon Cope, Keith Chan, Harlan Campbell, Jenny Chen, John Borrill, Jessica R May, William Malcolm, Sebastien Branchoux, Katrin Kupas, and Jeroen P Jansen. A comparison of alternative network meta-analysis methods in the presence of nonproportional hazards: a case study in first-line advanced or metastatic renal cell carcinoma.V alue in Health, 26(4):465...
work page 2023
-
[2]
Ian Koblbauer, Daniel Prieto-Alhambra, Edward Burn, and Rafael Pinedo-Villanueva. Applying trial-derived treatment effects to real-world populations: Generalizing cost-effectiveness estimates when modeling complex hazards.V alue in Health, 27:173–181, 2024
work page 2024
-
[3]
Jeroen P Jansen. Network meta-analysis of survival data with fractional polynomials.BMC medical research methodology, 11(1):61, 2011
work page 2011
-
[4]
Patricia Guyot, AE Ades, Mario JNM Ouwens, and Nicky J Welton. Enhanced secondary analysis of survival data: reconstructing the data from published kaplan-meier survival curves.BMC medical research methodology, 12(1):9, 2012
work page 2012
-
[5]
Network meta-analysis of parametric survival curves
Mario JNM Ouwens, Zoe Philips, and Jeroen P Jansen. Network meta-analysis of parametric survival curves. Research synthesis methods, 1(3-4):258–271, 2010
work page 2010
-
[6]
Jansen, Sven Klijn, Kevin Towle, Bill Malcolm, and Shannon Cope
Harlan Campbell, Dylan Maciel, Keith Chan, Jeroen P. Jansen, Sven Klijn, Kevin Towle, Bill Malcolm, and Shannon Cope. One-step parametric network meta-analysis models using the exact likelihood that allow for time-varying treatment effects.Research Synthesis Methods, 16(4):650–671, 2025
work page 2025
-
[7]
Suzanne C Freeman and James R Carpenter. Bayesian one-step ipd network meta-analysis of time-to-event data using royston-parmar models.Research synthesis methods, 8(4):451–464, 2017
work page 2017
-
[8]
Suzanne C Freeman, Alex J Sutton, Nicola J Cooper, Alessandro Gasparini, Michael J Crowther, and Neil Hawkins. Bayesian pairwise meta-analysis of time-to-event outcomes in the presence of non-proportional haz- ards: A simulation study of flexible parametric, piecewise exponential and fractional polynomial models.Re- search Synthesis Methods, 15(5):780–801, 2024
work page 2024
-
[9]
David M Phillippo, Ayman Sadek, Hugo Pedder, and Nicky J Welton. Network meta-analysis of survival out- comes with non-proportional hazards using flexible m-splines.arXiv preprint arXiv:2509.10383, 2025
-
[10]
Valentijn M.T. de Jong, Karel G.M. Moons, Richard D. Riley, Catrin Tudur Smith, Anthony G. Marson, Mari- nus J.C. Eijkemans, and Thomas P.A. Debray. Individual participant data meta-analysis of intervention studies with time-to-event outcomes: A review of the methodology and an applied example.Research Synthesis Meth- ods, 11(2):148–168, 2020
work page 2020
-
[11]
Laura A Trigg, GJ Melendez-Torres, Ahmed Abdelsabour, and Dawn Lee. Treatment effect waning assumptions: a review of national institute of health and care excellence technology appraisals.V alue in Health, 27(8):1003– 1011, 2024
work page 2024
-
[12]
Using time dependent covariates and time dependent coefficients in the cox model
Terry Therneau, Cynthia Crowson, and Elizabeth Atkinson. Using time dependent covariates and time dependent coefficients in the cox model. CRAN, Dec 2024
work page 2024
-
[13]
GASTRIC Group. Role of chemotherapy for advanced/recurrent gastric cancer: An individual-patient-data meta- analysis.European Journal of Cancer, 49:1565–1577, 2013
work page 2013
-
[14]
Federico Rotolo, Xavier Paoletti, and Stefan Michiels. surrosurv: An r package for the evaluation of failure time surrogate endpoints in individual patient data meta-analyses of randomized clinical trials.Computer methods and programs in biomedicine, 155:189–198, 2018
work page 2018
-
[15]
Peter C Austin. Statistical power to detect violation of the proportional hazards assumption when using the cox regression model.Journal of statistical computation and simulation, 88(3):533–552, 2018. 14 Meta-Analysis and Network Meta-Analysis with Time-V arying HRsOwen & Abrams
work page 2018
-
[16]
Michael J Zoratti, Tahira Devji, Oren Levine, Lehana Thabane, and Feng Xie. Network meta-analysis of therapies for previously untreated advanced braf-mutated melanoma.Cancer Treatment Reviews, 74:43–48, 2019
work page 2019
-
[17]
Suzanne C Freeman, Nicola J Cooper, Alex J Sutton, Michael J Crowther, James R Carpenter, and Neil Hawkins. Challenges of modelling approaches for network meta-analysis of time-to-event outcomes in the presence of non- proportional hazards to aid decision making: Application to a melanoma network.Statistical Methods in Medical Research, 31(5):839–861, 2022
work page 2022
-
[18]
David Collett.Modelling survival data in medical research. Chapman and Hall/CRC, 2023
work page 2023
-
[19]
R Foundation for Statistical Comput- ing, Vienna, Austria, 2026
R Core Team.R: A Language and Environment for Statistical Computing. R Foundation for Statistical Comput- ing, Vienna, Austria, 2026
work page 2026
-
[20]
David J Spiegelhalter, Keith R Abrams, and Jonathan P Myles.Bayesian approaches to clinical trials and health-care evaluation. John Wiley & Sons, 2004
work page 2004
-
[21]
Schmid, Heinz Schmidli, Sibylle Sturtz, Sebastian Weber, and Tim Friede
Christian R ¨over, Ralf Bender, Sofia Dias, Christopher H. Schmid, Heinz Schmidli, Sibylle Sturtz, Sebastian Weber, and Tim Friede. On weakly informative prior distributions for the heterogeneity parameter in bayesian random-effects meta-analysis.Research Synthesis Methods, 12(4):448–474, 2021
work page 2021
-
[22]
Alex J Sutton and Keith R Abrams. Bayesian methods in meta-analysis and evidence synthesis.Statistical methods in medical research, 10(4):277–303, 2001
work page 2001
-
[23]
Yinghui Wei and Julian PT Higgins. Bayesian multivariate meta-analysis with multiple outcomes.Statistics in medicine, 32(17):2911–2934, 2013
work page 2013
-
[24]
Andrew Gelman. Prior distributions for variance parameters in hierarchical models.Bayesian Analysis, 1(3):515–533, 2006
work page 2006
-
[25]
Thomas Lumley. Network meta-analysis for indirect treatment comparisons.Statistics in medicine, 21(16):2313– 2324, 2002
work page 2002
-
[26]
Felix A Achana, Nicola J Cooper, Sylwia Bujkiewicz, Stephanie J Hubbard, Denise Kendrick, David R Jones, and Alex J Sutton. Network meta-analysis of multiple outcome measures accounting for borrowing of informa- tion across outcomes.BMC medical research methodology, 14(1):1, 2014
work page 2014
-
[27]
JAGS: A program for analysis of bayesian graphical models using gibbs sampling
Martyn Plummer. JAGS: A program for analysis of bayesian graphical models using gibbs sampling. InProceed- ings of the 3rd International Workshop on Distributed Statistical Computing (DSC 2003), pages 1–10, Vienna, Austria, 2003
work page 2003
-
[28]
Martyn Plummer.rjags: Bayesian Graphical Models using MCMC, 2025. R package version 4-17
work page 2025
-
[29]
Inference from iterative simulation using multiple sequences.Statistical Science, 7(4):457–472, 1992
Andrew Gelman and Donald B Rubin. Inference from iterative simulation using multiple sequences.Statistical Science, 7(4):457–472, 1992
work page 1992
-
[30]
Aki Vehtari, Andrew Gelman, Daniel Simpson, Bob Carpenter, and Paul-Christian B¨urkner. Rank-normalization, folding, and localization: An improved ˆRfor assessing convergence of MCMC.Bayesian Analysis, 16(2):667– 718, 2021
work page 2021
-
[31]
CODA: Convergence diagnosis and output anal- ysis for MCMC.R News, 6(1):7–11, 2006
Martyn Plummer, Nicky Best, Kate Cowles, and Karen Vines. CODA: Convergence diagnosis and output anal- ysis for MCMC.R News, 6(1):7–11, 2006
work page 2006
-
[32]
Taddele Kibret, Danielle Richer, and Joseph Beyene. Bias in identification of the best treatment in a bayesian network meta-analysis for binary outcome: a simulation study.Clinical epidemiology, pages 451–460, 2014
work page 2014
-
[33]
David M Phillippo, Sofia Dias, AE Ades, Mark Belger, Alan Brnabic, Alexander Schacht, Daniel Saure, Zbig- niew Kadziola, and Nicky J Welton. Multilevel network meta-regression for population-adjusted treatment com- parisons.Journal of the Royal Statistical Society Series A: Statistics in Society, 183(3):1189–1210, 2020
work page 2020
-
[34]
Nicholas R Latimer and Amanda I Adler. Extrapolation beyond the end of trials to estimate long term survival and cost effectiveness.BMJ medicine, 1(1):e000094, 2022
work page 2022
-
[35]
Elizabeth A Handorf, Marc C Smaldone, Sujana Movva, and Nandita Mitra. Analysis of survival data with nonproportional hazards: A comparison of propensity-score-weighted methods.Biometrical journal, 66(1):202200099, 2024
work page 2024
-
[36]
Danielle L Burke, Joie Ensor, and Richard D Riley. Meta-analysis using individual participant data: one-stage and two-stage approaches, and why they may differ.Statistics in medicine, 36(5):855–875, 2017
work page 2017
-
[37]
Basia Rogula, Greta Lozano-Ortega, and Karissa M Johnston. A method for reconstructing individual patient data from kaplan-meier survival curves that incorporate marked censoring times.MDM Policy & Practice, 7(1), 2022. 15 Meta-Analysis and Network Meta-Analysis with Time-V arying HRsOwen & Abrams
work page 2022
-
[38]
Angus C Jennings, Mark J Rutherford, and Paul C Lambert. A spline-based approach to smoothly constrain hazard ratios with a view to apply treatment effect waning.Statistics in Medicine, 44(6):e70035, 2025
work page 2025
-
[39]
Nicholas R Latimer. Survival analysis for economic evaluations alongside clinical trials—extrapolation with patient-level data: inconsistencies, limitations, and a practical guide.Medical Decision Making, 33(6):743–754, 2013
work page 2013
-
[40]
Rhiannon K Owen, Douglas G Tincello, and R Abrams Keith. Network meta-analysis: development of a three- level hierarchical modeling approach incorporating dose-related constraints.V alue in Health, 18(1):116–126, 2015
work page 2015
-
[41]
Thomas Leahy, Megan Besford, and Cormac Sammon. Pmu109 how do nice evidence review groups and ap- praisal committees perceive fractional polynomial methodology in technology appraisals?V alue in Health, 22:S727, 2019
work page 2019
-
[42]
Svenja Petersohn, Bradley McGregor, Sven L Klijn, Jessica R May, Flavia Ejzykowicz, Murat Kurt, Matthew Dyer, Bill Malcolm, S ´ebastien Branchoux, Katharina Nickel, et al. Challenges in conducting fractional poly- nomial and standard parametric network meta-analyses of immune checkpoint inhibitors for first-line advanced renal cell carcinoma.Journal of Co...
work page 2023
-
[43]
Yinghui Wei, Patrick Royston, Jayne F Tierney, and Mahesh KB Parmar. Meta-analysis of time-to-event out- comes from randomized trials using restricted mean survival time: application to individual participant data. Statistics in Medicine, 34(21):2881–2898, 2015
work page 2015
-
[44]
Michael J Crowther, Richard D Riley, Jan A Staessen, Jiguang Wang, Francois Gueyffier, and Paul C Lambert. Individual patient data meta-analysis of survival data using poisson regression models.BMC Medical Research Methodology, 12(1):34, 2012
work page 2012
-
[45]
Philip Cooney and Arthur White. Extending beyond bagust and beale: Fully parametric piecewise exponential models for extrapolation of survival outcomes in health technology assessment.V alue in Health, 26(10):1510– 1517, 2023
work page 2023
-
[46]
Nicholas Latimer. Nice dsu technical support document 14: survival analysis for economic evaluations alongside clinical trials-extrapolation with patient-level data.Report by the decision support unit, 20, 2011
work page 2011
-
[47]
Therneau.coxme: Mixed Effects Cox Models, 2024
Terry M. Therneau.coxme: Mixed Effects Cox Models, 2024. R package version 2.2-22. 16 Meta-Analysis and Network Meta-Analysis with Time-V arying HRsOwen & Abrams Supplementary Materials S1 Pairwise meta-analysis - Advanced Gastric Cancer −4 −3 −2 −1 0 1 2 0.021 0.082 0.15 0.23 0.32 0.47 0.71 0.91 Time Beta(t) for tx Study 1 −4 −3 −2 −1 0 1 2 0.08 0.13 0.2...
work page 2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.