Recognition: 2 theorem links
· Lean TheoremReal-Time Surrogate Modeling for Personalized Blood Flow Prediction and Hemodynamic Analysis
Pith reviewed 2026-05-13 20:14 UTC · model grok-4.3
The pith
A neural surrogate model predicts patient-specific arterial pressure and cardiac output instantaneously from limited inputs.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
A deep neural surrogate trained on a parametrically generated virtual cohort that respects observed multivariate correlations from clinical data can map patient-specific input parameters to arterial pressure waveforms and cardiac output in a single forward pass, while also furnishing a sampling rule for terminal resistance that reduces uncertainty in unobservable parameters and revealing the minimal clinical measurements sufficient to solve the inverse problem for cardiac output.
What carries the argument
Deep neural surrogate model trained on a virtual cohort derived from multivariate clinical correlations, which maps input parameters directly to hemodynamic outputs.
If this is right
- Real-time prediction replaces repeated full simulations for screening large parameter spaces or generating hypertensive subgroups.
- Principled sampling of terminal resistance reduces the fraction of discarded synthetic cases and lowers uncertainty in unmeasurable parameters.
- The identified minimal measurement set shows which clinical variables carry the information needed to invert for cardiac output.
- Direct application to real patient data yields estimates of central aortic systolic pressure and cardiac output without additional invasive measurements.
Where Pith is reading between the lines
- The same surrogate architecture could be retrained on other 1-D or 3-D vascular domains to accelerate personalized simulations beyond the aorta.
- Embedding the model in a clinical workflow would allow immediate feedback on proposed parameter sets during patient intake.
- If distribution shift appears in new populations, lightweight fine-tuning on a small local cohort could restore accuracy without regenerating the entire virtual dataset.
Load-bearing premise
The multivariate correlations seen in the Asklepios dataset are representative enough of real physiological variation that a network trained on the resulting virtual cohort will generalize without major error to new clinical cases.
What would settle it
Apply the trained surrogate to an independent clinical cohort with measured cardiac output and central pressures; if the predicted values deviate systematically from the measured ones by more than the error tolerance reported in the paper, the generalization claim does not hold.
Figures





read the original abstract
Cardiovascular modeling has rapidly advanced over the past few decades due to the rising needs for health tracking and early detection of cardiovascular diseases. While 1-D arterial models offer an attractive compromise between computational efficiency and solution fidelity, their application on large populations or for generating large \emph{in silico} cohorts remains challenging. Certain hemodynamic parameters like the terminal resistance/compliance, are difficult to clinically estimate and often yield non-physiological hemodynamics when sampled naively, resulting in large portions of simulated datasets to be discarded. In this work, we present a systematic framework for training machine learning (ML) models, capable of instantaneous hemodynamic prediction and parameter estimation. We initially start with generating a parametric virtual cohort of patients which is based on the multivariate correlations observed in the large Asklepios clinical dataset, ensuring that physiological parameter distributions are respected. We then train a deep neural surrogate model, able to predict patient-specific arterial pressure and cardiac output (CO), enabling rapid a~priori screening of input parameters. This allows for immediate rejection of non-physiological combinations and drastically reduces the cost of targeted synthetic dataset generation (e.g. hypertensive groups). The model also provides a principled means of sampling the terminal resistance to minimize the uncertainties of unmeasurable parameters. Moreover, by assessing the model's predictive performance we determine the theoretical information which suffices for solving the inverse problem of estimating the CO. Finally, we apply the surrogate on a clinical dataset for the estimation of central aortic hemodynamics i.e. the CO and aortic systolic blood pressure (cSBP).
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents a framework for generating a virtual patient cohort from multivariate correlations in the Asklepios dataset and training a deep neural network surrogate model to predict patient-specific arterial pressure and cardiac output in real time. The surrogate enables efficient screening of input parameters to reject non-physiological combinations, provides a method for sampling terminal resistance, identifies sufficient information for inverse CO estimation, and is applied to estimate CO and central systolic blood pressure on a clinical dataset.
Significance. If the surrogate demonstrates accurate generalization from the virtual cohort to real clinical data with quantified error metrics, this work could substantially reduce the computational burden of 1D arterial modeling for large cohorts and enable real-time personalized hemodynamic analysis, with implications for clinical decision support in cardiovascular disease monitoring. The integration of data-driven surrogates with physiological constraints from clinical statistics is a promising direction.
major comments (3)
- The central claim that the DNN surrogate trained on the Asklepios-derived virtual cohort generalizes to real clinical data for instantaneous arterial pressure and CO prediction (and subsequent inverse CO estimation) lacks reported quantitative validation metrics such as MAE, R², or error bars against the underlying 1D solver on held-out simulated or clinical data; this is load-bearing for both the forward prediction and inverse-problem claims.
- No quantitative assessment of distribution shift (e.g., statistical comparison of input parameter distributions such as age, resistance values, or output hemodynamics) is provided between the Asklepios multivariate correlations used for cohort generation and the target clinical dataset, which directly risks invalidating the generalization and non-physiological sample rejection steps.
- The assertion that the model's predictive performance determines 'the theoretical information which suffices for solving the inverse problem of estimating the CO' requires explicit methodology details (e.g., feature ablation results or sensitivity analysis on which inputs enable accurate CO recovery) to support the claim; without this, the information-sufficiency conclusion remains unsubstantiated.
minor comments (2)
- The abstract contains the notation 'a~priori' which appears to be a typographical error for 'a priori'.
- The manuscript would benefit from clearer reporting of any performance metrics with variability measures (standard deviations or confidence intervals) to strengthen interpretability of results.
Simulated Author's Rebuttal
We thank the referee for their thoughtful and constructive review. The comments highlight important aspects of validation and methodological clarity that strengthen the manuscript. We address each major comment below and have revised the paper to incorporate quantitative metrics, distribution comparisons, and explicit ablation analyses where these were previously insufficiently detailed.
read point-by-point responses
-
Referee: The central claim that the DNN surrogate trained on the Asklepios-derived virtual cohort generalizes to real clinical data for instantaneous arterial pressure and CO prediction (and subsequent inverse-problem claims) lacks reported quantitative validation metrics such as MAE, R², or error bars against the underlying 1D solver on held-out simulated or clinical data; this is load-bearing for both the forward prediction and inverse-problem claims.
Authors: We agree that explicit quantitative validation metrics were not presented with sufficient detail in the original submission. In the revised manuscript we have added a new validation subsection reporting MAE, RMSE, and R² values (with standard deviations across five independent training runs) for both pressure waveforms and CO on a held-out portion of the virtual cohort. We also include direct comparison against the 1D solver on the same test cases. For the clinical dataset application we now report mean absolute errors and Pearson correlations for estimated CO and central systolic pressure against available reference values, together with error bars. These additions directly support the generalization and inverse-problem claims. revision: yes
-
Referee: No quantitative assessment of distribution shift (e.g., statistical comparison of input parameter distributions such as age, resistance values, or output hemodynamics) is provided between the Asklepios multivariate correlations used for cohort generation and the target clinical dataset, which directly risks invalidating the generalization and non-physiological sample rejection steps.
Authors: We acknowledge the absence of a formal distribution-shift analysis. The revised manuscript now includes a dedicated supplementary table and figure that compare key marginal and joint distributions (age, body surface area, terminal resistances, and resulting mean arterial pressure) between the Asklepios-derived virtual cohort and the clinical dataset. We report two-sample Kolmogorov-Smirnov statistics and p-values for each parameter, along with overlaid histograms. While the distributions show substantial overlap, we also discuss the modest differences observed in resistance ranges and their implications for the rejection step. revision: yes
-
Referee: The assertion that the model's predictive performance determines 'the theoretical information which suffices for solving the inverse problem of estimating the CO' requires explicit methodology details (e.g., feature ablation results or sensitivity analysis on which inputs enable accurate CO recovery) to support the claim; without this, the information-sufficiency conclusion remains unsubstantiated.
Authors: The original text described the information-sufficiency conclusion qualitatively from observed performance differences across input configurations. We have expanded the methods and results sections with an explicit feature-ablation study. The revised manuscript now presents CO estimation accuracy (MAE and R²) when the model is given progressively reduced input sets (full pressure waveform, selected pressure points, heart rate only, etc.). These quantitative results identify the minimal sufficient feature set and are used to justify the information-sufficiency statement. revision: yes
Circularity Check
No significant circularity in surrogate training and inverse-problem workflow
full rationale
The paper generates a virtual cohort by sampling from multivariate correlations observed in the Asklepios clinical dataset, trains a DNN surrogate on forward 1-D hemodynamic simulations to predict pressure and CO, uses the surrogate for rapid parameter screening and terminal-resistance sampling, and applies it to clinical data for CO/cSBP estimation. The claim that predictive performance assessment determines sufficient information for the inverse CO problem follows directly from the trained forward map without reducing to a self-definitional tautology, a fitted parameter renamed as prediction, or any self-citation chain. No load-bearing step equates the claimed result to its inputs by construction; the workflow remains externally falsifiable via held-out simulation error and clinical validation.
Axiom & Free-Parameter Ledger
free parameters (1)
- terminal resistance and compliance values
axioms (1)
- domain assumption Multivariate correlations in the Asklepios dataset capture the full physiological range of arterial parameters
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
We then train a deep neural surrogate model, able to predict patient-specific arterial pressure and cardiac output (CO)... The model also provides a principled means of sampling the terminal resistance...
-
IndisputableMonolith/Foundation/AlphaCoordinateFixation.leanJ_uniquely_calibrated_via_higher_derivative unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
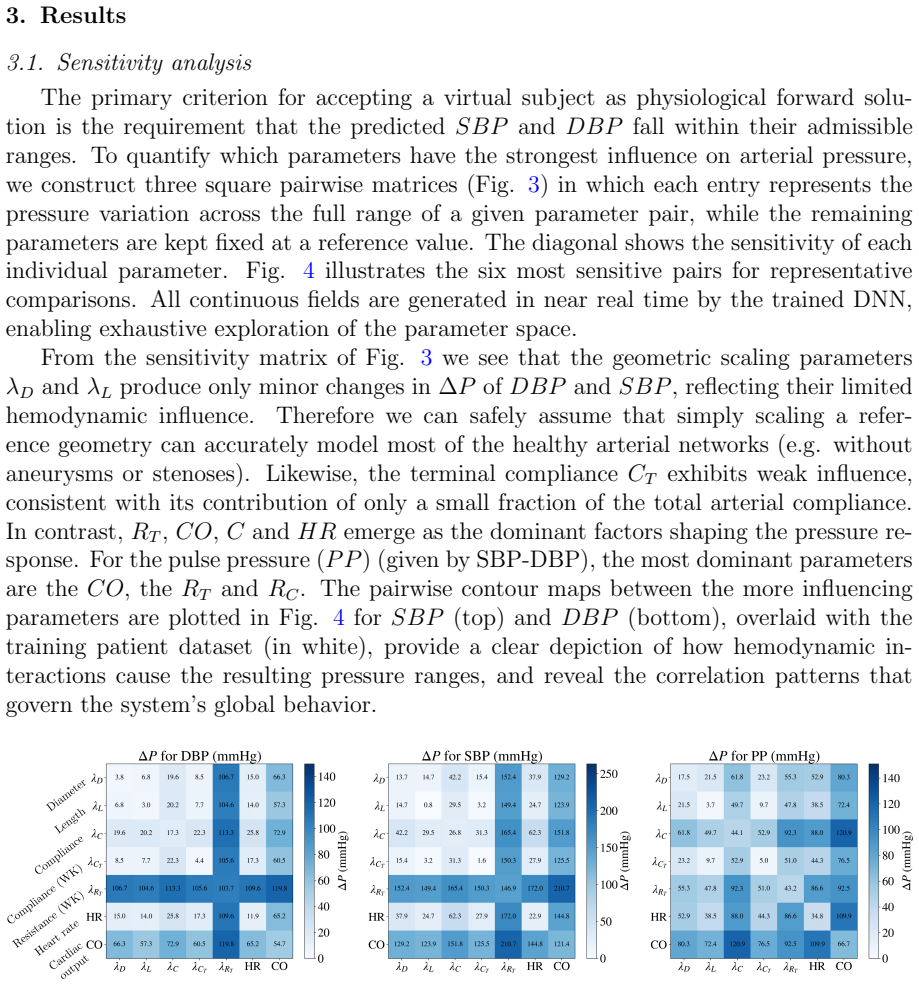
Pair-wise parameter sensitivity... dominant factors shaping the pressure response are RT, CO, C and HR
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Y. Shi, P. Lawford, D. R. Hose, Review of Zero-D and 1-D models of blood flow in the cardiovascular system, BioMedical Engineering OnLine 10 (2011) 33
work page 2011
-
[2]
L. Formaggia, D. Lamponi, A. Quarteroni, One-dimensional models for blood flow in arteries, Journal of Engineering Mathematics 47 (3-4) (2003) 251–276
work page 2003
-
[3]
S. J. Sherwin, V. Franke, J. Peir´ o, K. H. Parker, One-dimensional modelling of a vascular network in space-time variables, Journal of Engineering Mathematics 47 (3-
-
[4]
K. S. Matthys, J. Alastruey, J. Peir´ o, A. W. Khir, P. Segers, P. R. Verdonck, K. H. Parker, S. J. Sherwin, Pulse wave propagation in a model human arterial network: Assessment of 1-D numerical simulations against in vitro measurements, Journal of Biomechanics 40 (15) (2007) 3476–3486
work page 2007
-
[5]
P. Reymond, F. Merenda, F. Perren, D. Rufenacht, N. Stergiopulos, Validation of a one-dimensional model of the systemic arterial tree, American Journal of Physiology- Heart and Circulatory Physiology 297 (1) (2009) H208–H222
work page 2009
-
[6]
J. Alastruey, K. H. Parker, J. Peir´ o, S. J. Sherwin, Analysing the pattern of pulse waves in arterial networks: A time-domain study, Journal of Engineering Mathemat- ics 64 (2009) 331–351
work page 2009
-
[7]
V. Bikia, S. Pagoulatou, B. Trachet, D. Soulis, A. D. Protogerou, T. G. Papaioannou, N. Stergiopulos, Noninvasive cardiac output and central systolic pressure from cuff- pressure and pulse wave velocity, IEEE journal of biomedical and health informatics 24 (7) (2019) 1968–1981
work page 2019
-
[8]
S. Laurent, J. Cockcroft, L. Van Bortel, P. Boutouyrie, C. Giannattasio, D. Hayoz, B. Pannier, C. Vlachopoulos, I. Wilkinson, H. Struijker-Boudier, et al., Expert con- sensus document on arterial stiffness: Methodological issues and clinical applications, European Heart Journal 27 (21) (2006) 2588–2605
work page 2006
-
[9]
L. M. Van Bortel, S. Laurent, P. Boutouyrie, P. Chowienczyk, J. K. Cruickshank, T. De Backer, J. Filipovsk´ y, S. Huybrechts, F. U. S. Mattace-Raso, A. D. Protogerou, et al., Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity, Journal of Hypertension 30 (3) (2012) 445–448
work page 2012
-
[10]
M. R. Pfaller, J. Pham, A. Verma, L. Pegolotti, N. M. Wilson, D. W. Parker, W. Yang, A. L. Marsden, Automated generation of 0D and 1D reduced-order mod- els of patient-specific blood flow, International Journal for Numerical Methods in Biomedical Engineering 38 (10) (2022) e3639. 17
work page 2022
-
[11]
L. Pegolotti, M. R. Pfaller, N. L. Rubio, K. Ding, R. Brugarolas Brufau, E. Darve, A. L. Marsden, Learning reduced-order models for cardiovascular simulations with graph neural networks, Computers in Biology and Medicine 168 (2024) 107676
work page 2024
-
[12]
V. Bikia, G. Rovas, S. Pagoulatou, N. Stergiopulos, Determination of aortic charac- teristic impedance and total arterial compliance from regional pulse wave velocities using machine learning: an in-silico study, Frontiers in bioengineering and biotech- nology 9 (2021) 649866
work page 2021
- [13]
- [14]
-
[15]
E. R. Rietzschel, M. L. De Buyzere, S. Bekaert, P. Segers, D. De Bacquer, L. Cooman, P. Van Damme, P. Cassiman, M. Langlois, P. Van Oostveldt, et al., Rationale, design, methods and baseline characteristics of the Asklepios study, European Journal of Cardiovascular Prevention & Rehabilitation 14 (2) (2007) 179–191
work page 2007
-
[16]
M. D. McKay, R. J. Beckman, W. J. Conover, A comparison of three methods for selecting values of input variables in the analysis of output from a computer code, Technometrics 21 (2) (1979) 239–245
work page 1979
-
[17]
G. J. Langewouters, Visco-elasticity of the human aorta in vitro in relation to pressure and age, Ph.D. thesis, Krips Repro (1982)
work page 1982
-
[18]
P. Segers, E. Rietzschel, M. De Buyzere, N. Stergiopulos, N. Westerhof, L. Van Bor- tel, T. Gillebert, P. Verdonck, Three-and four-element windkessel models: assessment of their fitting performance in a large cohort of healthy middle-aged individuals, Pro- ceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine 222 ...
work page 2008
-
[19]
Z. Lu, R. Mukkamala, Continuous cardiac output monitoring in humans by invasive and noninvasive peripheral blood pressure waveform analysis, Journal of Applied Physiology 101 (2) (2006) 598–608
work page 2006
-
[20]
A. Wolak, H. Gransar, L. E. Thomson, J. D. Friedman, R. Hachamovitch, A. Gut- stein, L. J. Shaw, D. Polk, N. D. Wong, R. Saouaf, et al., Aortic size assessment by noncontrast cardiac computed tomography: normal limits by age, gender, and body surface area, JACC: Cardiovascular Imaging 1 (2) (2008) 200–209
work page 2008
-
[21]
P. Segers, E. R. Rietzschel, M. L. D. Buyzere, S. J. Vermeersch, D. D. Bacquer, L. M. V. Bortel, G. D. Backer, T. C. Gillebert, P. R. Verdonck, Noninvasive (input) impedance, pulse wave velocity, and wave reflection in healthy middle-aged men and women, Hypertension 49 (6) (2007) 1248–1255. 18
work page 2007
-
[22]
E.-R. Rietzschel, M. L. De Buyzere, S. Bekaert, P. Segers, D. De Bacquer, L. Cooman, P. Van Damme, P. Cassiman, M. Langlois, P. van Oostveldt, P. Ver- donck, G. De Backer, T. C. Gillebert, the Asklepios investigators, Rationale, design, methods and baseline characteristics of the asklepios study, European journal of car- diovascular prevention and rehabil...
work page 2007
-
[23]
E.-R. Rietzschel, M. L. De Buyzere, S. Bekaert, P. Segers, D. De Bacquer, L. Cooman, P. Van Damme, P. Cassiman, M. Langlois, P. van Oostveldt, et al., Rationale, design, methods and baseline characteristics of the asklepios study, European Journal of Preventive Cardiology 14 (2) (2007) 179–191
work page 2007
-
[24]
T. G. Papaioannou, D. Soulis, O. Vardoulis, A. Protogerou, P. P. Sfikakis, N. Ster- giopulos, C. Stefanadis, First in vivo application and evaluation of a novel method for non-invasive estimation of cardiac output, Medical engineering & physics 36 (10) (2014) 1352–1357. 19
work page 2014
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.