Recognition: unknown
Measles Resurgence in Bangladesh, 2026: A Situational Analysis for Urgent Public Health Response
Pith reviewed 2026-05-08 12:51 UTC · model grok-4.3
The pith
Bangladesh's measles resurgence in 2026 stems from immunity gaps due to coverage declines and program disruptions, not vaccine failure.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
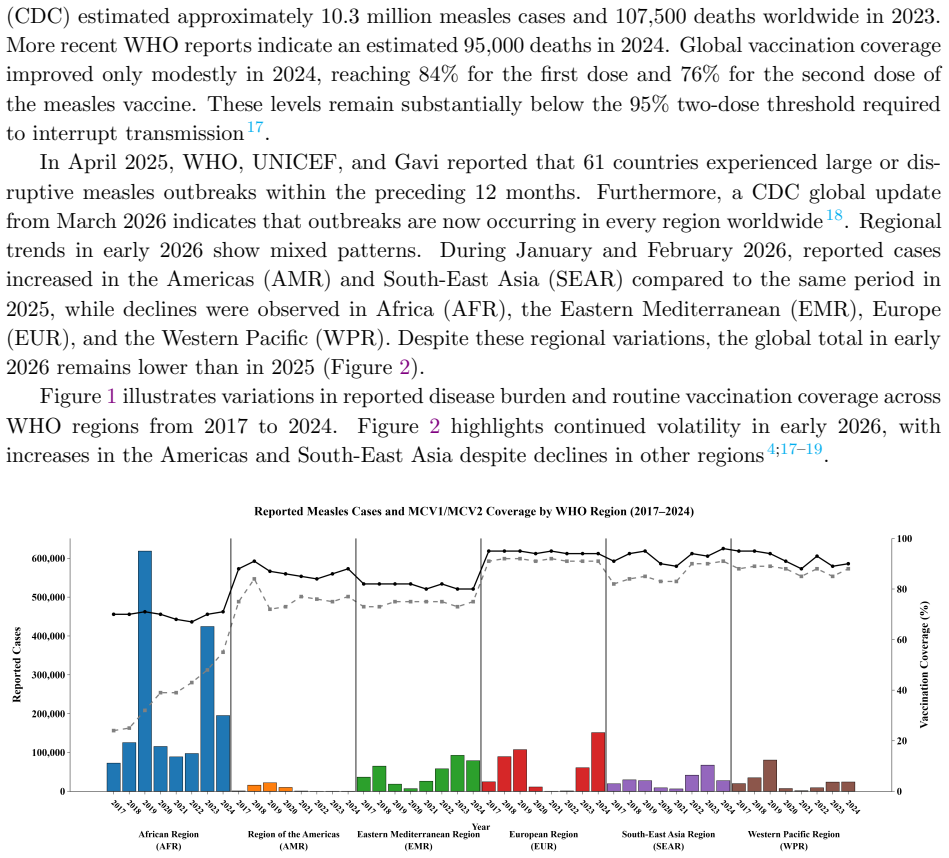
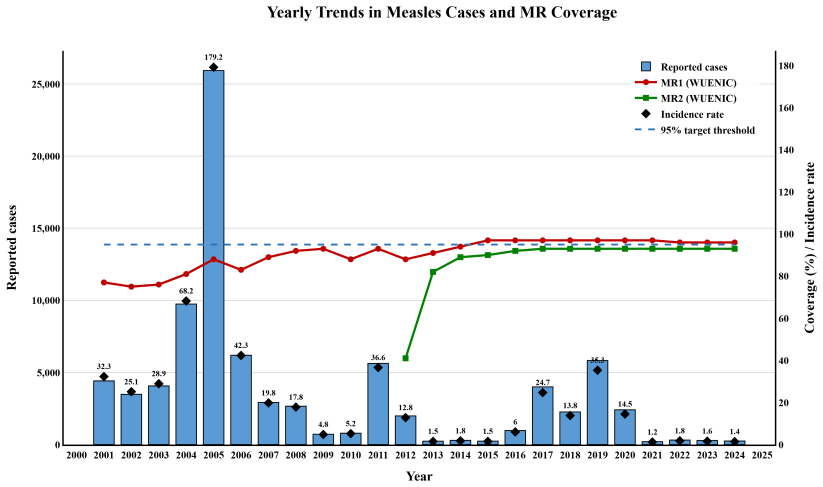
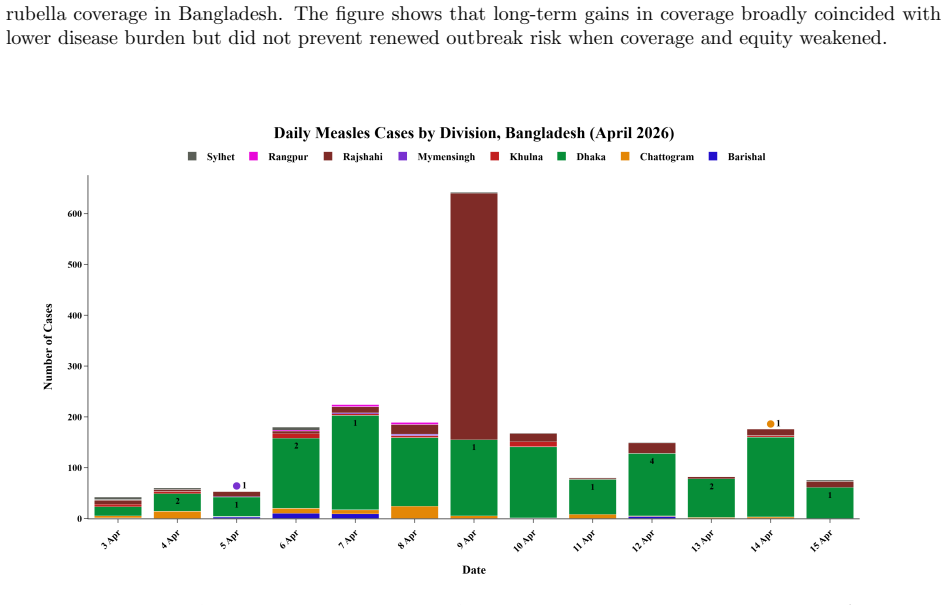
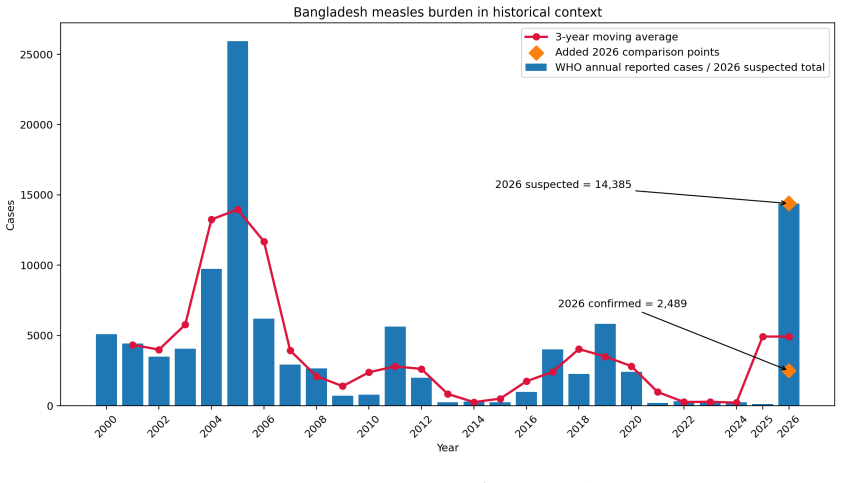
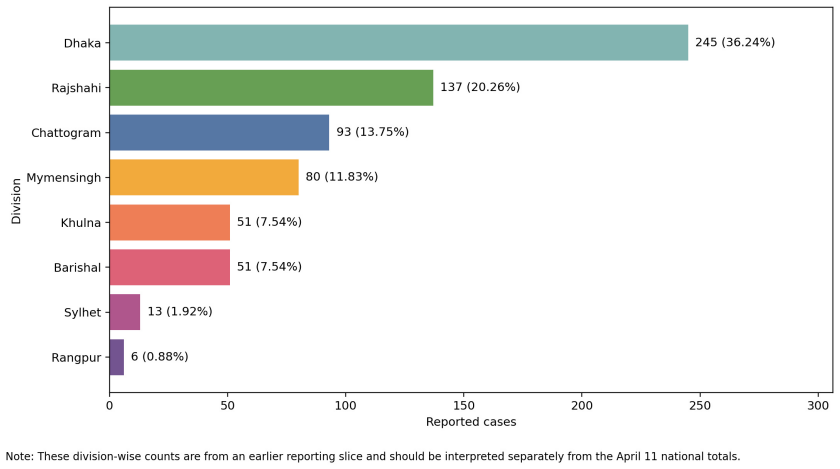
By mid-April 2026 Bangladesh had recorded 19,161 suspected measles cases, 2,973 confirmed cases, and 166 suspected deaths across 58 districts. The outbreak concentrated in two divisions that held 56.5 percent of cases, with children under five making up 81 percent and 72 percent of cases having received zero doses. National MR1 coverage fell from 88.6 percent to 86 percent and MR2 from 89 percent to 80.7 percent between 2019 and 2024, leaving roughly 20 million children vulnerable. The paper states that the resurgence reflects these accumulated immunity gaps from subnational inequities and programme disruption rather than vaccine failure.
What carries the argument
Rapid mixed-evidence review of aggregated surveillance data from WHO, UNICEF, DGHS, and media sources that tracks case counts, vaccination status, and coverage trends to identify immunity gaps as the transmission driver.
If this is right
- Targeted vaccination campaigns are required in the most affected divisions and among zero-dose children to close immunity gaps.
- Vitamin A supplementation must be restored as part of the outbreak response.
- Paediatric care capacity needs strengthening to manage severe cases and prevent deaths.
- Real-time surveillance should be integrated into ongoing outbreak response to guide further action.
Where Pith is reading between the lines
- Other countries recovering from pandemic-related immunization disruptions may face similar concentrated outbreaks if subnational coverage inequities are not addressed.
- Focusing recovery efforts on the lowest-coverage districts rather than uniform national targets could interrupt transmission more efficiently.
- Follow-up studies measuring case incidence after targeted campaigns would test whether closing the identified zero-dose gaps reduces spread as expected.
Load-bearing premise
The aggregated surveillance data from WHO, UNICEF, DGHS, and media sources accurately captures true case numbers, vaccination status, and causes without major underreporting, misdiagnosis, or selection bias.
What would settle it
Finding that a large share of confirmed cases had received two valid doses of measles-rubella vaccine, or detecting vaccine-escape virus variants in sequenced samples from the outbreak, would indicate vaccine failure rather than immunity gaps.
Figures




read the original abstract
\textbf{Background} Measles has resurged globally in the post-pandemic period as routine immunisation recovery remains below the two-dose threshold required to interrupt transmission. Bangladesh, previously nearing measles--rubella elimination, entered 2026 with widening coverage gaps, depleted vaccine stocks, and increasing numbers of missed children. We conducted a situation analysis to assess the scale, concentration, and programmatic implications of the outbreak. \textbf{Methods} We performed a rapid mixed-evidence review from 1--15 April 2026 using data from WHO, UNICEF, DGHS bulletins, PubMed/MEDLINE, ReliefWeb, SEARO updates, and Bangla-language media. Of 46 records screened, 19 were included. Analysis was based on aggregated, publicly available surveillance and programme data. \textbf{Findings} By 15 April 2026, Bangladesh reported 19{,}161 suspected cases, 2{,}973 confirmed cases, 166 suspected deaths, and 32 confirmed deaths across 58 districts since 15 March 2026. The outbreak was spatially concentrated: the top two divisions accounted for 56.5\% of cases (HHI = 0.217). Children under five comprised 81\% of cases, including 34\% infants under nine months. Vaccination status showed 72\% zero-dose and 16\% partially vaccinated cases. Coverage declined from 88.6\% to 86\% for MR1 and from 89\% to 80.7\% for MR2 (2019--2024), leaving about 20 million children vulnerable. \textbf{Interpretation} The resurgence reflects accumulated immunity gaps rather than vaccine failure, driven by subnational inequities and programme disruption. Urgent priorities include targeted vaccination campaigns, restoration of vitamin A supplementation, strengthening paediatric care capacity, and integrating real-time surveillance into outbreak response.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript conducts a rapid mixed-evidence review of publicly available data to describe a measles resurgence in Bangladesh starting March 2026. It reports 19,161 suspected cases and 2,973 confirmed cases across 58 districts, with 81% of cases in children under five, 72% zero-dose, and 16% partially vaccinated. The analysis concludes that the outbreak is driven by accumulated immunity gaps from declining MR1 and MR2 coverage (to 86% and 80.7%) and subnational inequities, rather than vaccine failure, and outlines urgent response priorities.
Significance. If the surveillance data accurately reflect vaccination status and case ascertainment, this situational analysis offers a timely compilation of outbreak metrics that could guide immediate public health actions in Bangladesh and contribute to understanding post-pandemic measles dynamics. The use of the Herfindahl-Hirschman Index for spatial concentration and the quantification of vulnerable children provide concrete figures for planning. However, as a descriptive review without new empirical validation, its long-term scientific impact is modest compared to studies with primary data or modeling.
major comments (2)
- [Methods] The methods describe a rapid review of aggregated data from WHO, UNICEF, DGHS, PubMed, ReliefWeb, and media but provide no details on how vaccination status was ascertained or validated in the 2,973 confirmed cases (e.g., via immunization cards, registry linkage, or bias adjustment). This is load-bearing for the central claim in the Interpretation section that the resurgence reflects immunity gaps rather than vaccine failure, as media and aggregated reports often over-represent unvaccinated severe cases.
- [Findings / Interpretation] The assertion that the outbreak is due to immunity gaps 'rather than vaccine failure' relies solely on the observed vaccination status distribution (72% zero-dose, 16% partial) without presenting data on vaccine effectiveness, cold-chain integrity, or comparisons to expected attack rates in vaccinated populations. The 12% of cases with presumed full vaccination status could indicate failure or misclassification, but no analysis addresses this.
minor comments (2)
- [Abstract] The abstract uses LaTeX-style formatting for large numbers (e.g., 19{,}161); this should be rendered consistently as 19,161 in the published version for readability.
- [Full text] Ensure that all data sources are explicitly cited with dates and URLs where possible, as the rapid review includes media sources that may require verification.
Simulated Author's Rebuttal
We thank the referee for the constructive comments. We have revised the manuscript to address the concerns by expanding the Methods section on data provenance and by moderating the language in the Interpretation to reflect the descriptive, secondary-data nature of the analysis.
read point-by-point responses
-
Referee: [Methods] The methods describe a rapid review of aggregated data from WHO, UNICEF, DGHS, PubMed, ReliefWeb, and media but provide no details on how vaccination status was ascertained or validated in the 2,973 confirmed cases (e.g., via immunization cards, registry linkage, or bias adjustment). This is load-bearing for the central claim in the Interpretation section that the resurgence reflects immunity gaps rather than vaccine failure, as media and aggregated reports often over-represent unvaccinated severe cases.
Authors: We agree that the Methods section requires greater transparency. The vaccination status figures are taken directly from aggregated DGHS surveillance bulletins, which do not include the underlying case-investigation protocols or validation methods. We have revised the Methods to state explicitly that 'vaccination status is as reported in the aggregated surveillance data without independent verification' and have added a Limitations paragraph acknowledging potential reporting biases, including possible over-representation of unvaccinated severe cases, and the absence of bias-adjustment procedures. revision: yes
-
Referee: [Findings / Interpretation] The assertion that the outbreak is due to immunity gaps 'rather than vaccine failure' relies solely on the observed vaccination status distribution (72% zero-dose, 16% partial) without presenting data on vaccine effectiveness, cold-chain integrity, or comparisons to expected attack rates in vaccinated populations. The 12% of cases with presumed full vaccination status could indicate failure or misclassification, but no analysis addresses this.
Authors: The referee is correct that the original phrasing was overly definitive given the data available. The 12% of cases reported as fully vaccinated may represent vaccine failure, cold-chain compromise, or misclassification, none of which can be assessed with the aggregated sources used. We have revised the Interpretation to state that the resurgence is 'primarily driven by accumulated immunity gaps... although vaccine failure or misclassification cannot be excluded for a minority of cases.' We have also added a forward-looking statement on the need for vaccine-effectiveness studies in the response priorities section. revision: partial
Circularity Check
No circularity: purely descriptive compilation of external surveillance data with no derivations or self-referential steps
full rationale
The paper is a rapid mixed-evidence situational analysis that aggregates and interprets publicly reported numbers (suspected/confirmed cases, deaths, vaccination status, coverage trends) from independent external sources (WHO, UNICEF, DGHS, media). No equations, models, fitted parameters, predictions, or mathematical derivations appear anywhere. The central interpretation (resurgence reflects immunity gaps) is a direct reading of the observed 72% zero-dose and 16% partially-vaccinated distribution among confirmed cases, not a reduction of any output to its own inputs by construction. No self-citations, uniqueness theorems, or ansatzes are invoked to support load-bearing claims. This matches the default expectation of a non-circular descriptive report.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Immunization agenda 2030: Mid-point review
World Health Organization. Immunization agenda 2030: Mid-point review. Technical re- port, World Health Organization, Geneva, 2025. URLhttps://www.who.int/publications/ m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind. Ac- cessed 11 April 2026
2030
-
[2]
Measles deaths down 88% since 2000, but cases surge, November 2025
World Health Organization. Measles deaths down 88% since 2000, but cases surge, November 2025. URLhttps://www.who.int/news/item/ 28-11-2025-measles-deaths-down-88--since-2000--but-cases-surge. Accessed 11 April 2026
2000
-
[3]
World Health Organization and UNICEF. Progress and challenges with achieving universal immunization coverage: 2025 WUENIC estimates.https://data.unicef.org/resources/ data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=.IM_MCV1+IM_ MCV2..&startPeriod=2000&endPeriod=2024, July 2025. Accessed 11 April 2026
2025
-
[4]
WHO south-east Asia region epidemiological bulletin, 7th edition
World Health Organization Regional Office for South-East Asia. WHO south-east Asia region epidemiological bulletin, 7th edition. Technical report, WHO SEARO, New Delhi, April 2026. URLhttps://cdn.who.int/media/docs/default-source/searo/whe/wherepib/2026_07_ searo_epi_bulletin.pdf. Accessed 11 April 2026
2026
-
[5]
Progress toward measles elimination — Bangladesh, 2000–2016.MMWR Morbidity and Mortality Weekly Report, 66(28):753–757,
Sudhir Khanal, Rajendra Bohara, Stephen Chacko, Mohammad Sharifuzzaman, Mohammad Shamsuzzaman, James L Goodson, Alya Dabbagh, Katrina Kretsinger, Deepak Dhongde, Jayantha Liyanage, Sunil Bahl, and Arun Thapa. Progress toward measles elimination — Bangladesh, 2000–2016.MMWR Morbidity and Mortality Weekly Report, 66(28):753–757,
2000
-
[6]
doi: 10.15585/mmwr.mm6628a3
-
[7]
Md Jasim Uddin, Gourab Adhikary, Md Wazed Ali, Syed Ahmed, Mohammad Shamsuzza- man, Chris Odell, et al. Evaluation of impact of measles rubella campaign on vaccination 15 coverage and routine immunization services in Bangladesh.BMC Infectious Diseases, 16: 411, 2016. doi: 10.1186/s12879-016-1758-x. URLhttps://link.springer.com/article/ 10.1186/s12879-016-1758-x
-
[8]
Leaving no child behind: a step closer to elimina- tion of measles and rubella from Bangladesh, December 2020
World Health Organization Bangladesh. Leaving no child behind: a step closer to elimina- tion of measles and rubella from Bangladesh, December 2020. URLhttps://www.who.int/ bangladesh/news/detail/30-12-2020-leaving-no-child-behind. Accessed 11 April 2026
2020
-
[9]
Bangladesh: WHO and UNICEF estimates of immunization coverage: 2023 revision
World Health Organization and United Nations Children’s Fund. Bangladesh: WHO and UNICEF estimates of immunization coverage: 2023 revision. Technical report, WHO/UNICEF, Geneva/New York, July 2024. URLhttps://cdn.who.int/media/ docs/default-source/country-profiles/immunization/2024-country-profiles/ immunization-2024-bgd.pdf. Accessed 2026-04-21
2023
-
[10]
Lisa R. Feldstein et al. Vaccination coverage survey and seroprevalence among forcibly dis- placed rohingya children, cox’s bazar, bangladesh.PLOS Medicine, 2020. URLhttps: //journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003071
-
[11]
Global resurgence in measles.The Lancet Microbe, 2026
The Lancet Microbe. Global resurgence in measles.The Lancet Microbe, 2026. doi: 10.1016/ S2666-5247(26)00002-9. URLhttps://www.thelancet.com/journals/lanmic/article/ PIIS2666-5247(26)00002-9/fulltext. Accessed 11 April 2026
2026
-
[12]
Accelerating measles and rubella elimina- tion in Southeast Asia.The Lancet Regional Health – Southeast Asia, 2025
The Lancet Regional Health – Southeast Asia. Accelerating measles and rubella elimina- tion in Southeast Asia.The Lancet Regional Health – Southeast Asia, 2025. doi: 10.1016/ S2772-3682(25)00153-2. URLhttps://www.thelancet.com/journals/lansea/article/ PIIS2772-3682(25)00153-2/fulltext. Accessed 11 April 2026
2025
-
[13]
Measles outbreak in Bangladesh, 21 children dead in March, questions over vaccine shortage, March 2026
Shishir Moral. Measles outbreak in Bangladesh, 21 children dead in March, questions over vaccine shortage, March 2026. URLhttps://en.prothomalo.com/bangladesh/t7gt89boos. Prothom Alo (English edition); Accessed 11 April 2026
2026
-
[14]
Measles: 38 children dead in Bangladesh outbreak.BMJ, 393:s654, 2026
BMJ. Measles: 38 children dead in Bangladesh outbreak.BMJ, 393:s654, 2026. doi: 10.1136/ bmj.s654. URLhttps://www.bmj.com/content/393/bmj.s654. Accessed 11 April 2026
2026
-
[15]
Bangladesh measles outbreak situation report no
UNICEF Bangladesh. Bangladesh measles outbreak situation report no. 1, 08 april 2026. Technical report, UNICEF, April 2026. URLhttps://reliefweb.int/report/bangladesh/ unicef-bangladesh-measles-outbreak-situation-report-no-1-08-april-2026. Re- liefWeb posting. Accessed 11 April 2026
2026
-
[16]
Bangladesh faces vaccine shortage for 10 diseases: Health services secretary, March 2026
The Business Standard. Bangladesh faces vaccine shortage for 10 diseases: Health services secretary, March 2026. URLhttps://www.tbsnews.net/bangladesh/health/ bangladesh-faces-vaccine-shortage-10-diseases-health-secretary-1398836. Ac- cessed 11 April 2026
2026
-
[17]
Bangladesh launches measles vaccination drive as child death toll passes 100, April 2026
Hannah Ellis-Petersen. Bangladesh launches measles vaccination drive as child death toll passes 100, April 2026. URLhttps://www.theguardian.com/world/2026/apr/07/ bangladesh-measles-vaccination-drive-child-death-toll. The Guardian; Accessed 11 April 2026. 16
2026
-
[18]
Measles, November 2025
World Health Organization. Measles, November 2025. URLhttps://www.who.int/ news-room/fact-sheets/detail/measles. Updated 28 November 2025; Accessed 2026-04- 21
2025
-
[19]
Measles cases surge worldwide, infecting 10.3 million people in 2023, November 2024
World Health Organization. Measles cases surge worldwide, infecting 10.3 million people in 2023, November 2024. URLhttps://www.who.int/ news/item/14-11-2024-measles-cases-surge-worldwide--infecting-10. 3-million-people-in-2023. Accessed 2026-04-21
2023
-
[20]
WHO immunization data portal: Provisional measles and rubella data, 2026
World Health Organization. WHO immunization data portal: Provisional measles and rubella data, 2026. URLhttps://immunizationdata.who.int/global?location=&topic= Provisional-measles-and-rubella-data. Accessed 2026-04-21
2026
-
[21]
WHO south-east Asia region epidemiological bulletin
World Health Organization Regional Office for South-East Asia. WHO south-east Asia region epidemiological bulletin. Technical report, WHO SEARO, New Delhi, April 2026. URLhttps://cdn.who.int/media/docs/default-source/searo/whe/wherepib/2026_07_ searo_epi_bulletin.pdf. Accessed 2026-04-21
2026
-
[22]
Press releases, 2026
Directorate General of Health Services. Press releases, 2026. URLhttps://dghs.gov.bd/ pages/press-releases. Accessed 2026-04-21
2026
-
[23]
Frequently asked questions about measles in Bangladesh, April 2026
UNICEF Bangladesh. Frequently asked questions about measles in Bangladesh, April 2026. URLhttps://www.unicef.org/bangladesh/en/stories/ frequently-asked-questions-about-measles-bangladesh. Accessed 2026-04-21
2026
-
[24]
Nationwide response mobi- lized to contain measles outbreak in Bangladesh, April 2026
World Health Organization Regional Office for South-East Asia. Nationwide response mobi- lized to contain measles outbreak in Bangladesh, April 2026. URLhttps://www.who.int/ southeastasia/news/detail/15-04-2026-response-measlesBN. Accessed 2026-04-21
2026
-
[25]
Bangladesh humanitarian situation report no
UNICEF Bangladesh. Bangladesh humanitarian situation report no. 1 (measles outbreak). Technical report, UNICEF, Dhaka, April 2026. URLhttps://www.unicef.org/media/ 179846/file/Bangladesh-Humanitarian-Situation-Report-No.1%28Measles-Outbreak% 29-8-April-2026.pdf. Accessed 2026-04-21
2026
-
[26]
Press releases and daily measles surveil- lance bulletins.https://dghs.gov.bd/pages/press-releases, 2026
Directorate General of Health Services, Bangladesh. Press releases and daily measles surveil- lance bulletins.https://dghs.gov.bd/pages/press-releases, 2026. Accessed 11–15 April 2026
2026
-
[27]
Bangladesh launches emergency measles– rubella campaign with UNICEF, WHO and Gavi to protect over 1.2 million children, April 2026
World Health Organization Bangladesh. Bangladesh launches emergency measles– rubella campaign with UNICEF, WHO and Gavi to protect over 1.2 million children, April 2026. URLhttps://www.who.int/bangladesh/news/detail/ 05-04-2026-bangladesh-launches-emergency-measles-rubella-campaign-with-unicef--who-2-million-children. Accessed 11 April 2026
2026
-
[28]
BGD: Epidemic — 03-2026 — measles in Bangladesh
International Federation of Red Cross and Red Crescent Societies. BGD: Epidemic — 03-2026 — measles in Bangladesh. Technical report, IFRC GO, April 2026. URLhttps://go.ifrc. org/field-reports/18266. Accessed 11 April 2026. 17
2026
-
[29]
Bangladesh measles outbreak (dg echo, media, dghs, ifrc, unicef) - echo daily flash of 7 april 2026, 2026
ReliefWeb. Bangladesh measles outbreak (dg echo, media, dghs, ifrc, unicef) - echo daily flash of 7 april 2026, 2026. URLhttps://reliefweb.int/report/bangladesh/ bangladesh-measles-outbreak-dg-echo-media-dghs-ifrc-unicef-echo-daily-flash-7-april-2026. Accessed 2026-04-13
2026
-
[30]
Taylor Chin, Caroline O. Buckee, and Ayesha S. Mahmud. Quantifying the success of measles vaccination campaigns in the rohingya refugee camps.Epidemics, 30:100385, 2020. doi: 10.1016/j.epidem.2020.100385. URLhttps://www.sciencedirect.com/science/article/ pii/S1755436519301331. Open access via PubMed Central
-
[31]
Syed M. Akramuzzaman, Felicity T. Cutts, Md J. Hossain, Obaidullah K. Wahedi, Nazmun Nahar, Darul Islam, Narayan C. Shaha, and Dilip Mahalanabis. Measles vaccine effectiveness and risk factors for measles in Dhaka, Bangladesh.Bulletin of the World Health Organization, 80(10):776–782, 2002. doi: 10.1590/S0042-96862002001000005. URLhttps://pmc.ncbi.nlm. nih...
-
[32]
Takudzwa S. Sayi, Umid M. Sharapov, Zachary Matson, Melissa M. Coughlin, et al. Im- munogenicity and safety of a measles and rubella-containing vaccine at age 6 and 9 months in Bangladesh: an open-label, randomised trial.The Lancet Child & Adolescent Health, 9 (5):306–314, 2025. doi: 10.1016/S2352-4642(25)00090-2. URLhttps://www.sciencedirect. com/science...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.