Recognition: 2 theorem links
· Lean TheoremA Proof-of-Concept Simulation-Driven Digital Twin Framework for Decision-Aware Diabetes Modeling
Pith reviewed 2026-05-13 01:54 UTC · model grok-4.3
The pith
A proof-of-concept digital twin framework integrates prediction with counterfactual simulation to support decision-aware diabetes modeling using benchmark and synthetic data.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The paper establishes that a digital twin framework built on benchmark clinical data and synthetic temporal augmentation can generate interpretable simulated trajectories by merging predictive models with counterfactual simulation, thereby enabling decision-aware analysis of intervention effects in diabetes without asserting clinical accuracy.
What carries the argument
The simulation-driven digital twin framework, which merges predictive modeling with counterfactual simulation to produce decision-aware glucose trajectories from mixed real and synthetic data.
If this is right
- Prediction models become usable for generating alternative outcome paths rather than single forecasts.
- Intervention effects can be illustrated through controlled synthetic scenarios overlaid on real data patterns.
- The approach supplies a reusable structure for future simulation-driven systems in healthcare.
- Temporal behavior and decision impacts become visible in continuous glucose monitoring examples.
Where Pith is reading between the lines
- The same structure could be tested on other chronic conditions that rely on time-series physiological data.
- Linking the twin directly to live sensor streams might allow ongoing updates to the simulated trajectories.
- Quantitative comparison against long-term outcome registries would be required to assess how well the synthetic augmentations match reality.
Load-bearing premise
Benchmark clinical data plus controlled synthetic temporal augmentation can produce trajectories representative enough for meaningful decision-aware counterfactual analysis.
What would settle it
Demonstration that real patient glucose responses to the same interventions diverge substantially from the framework's simulated counterfactual trajectories.
Figures





read the original abstract
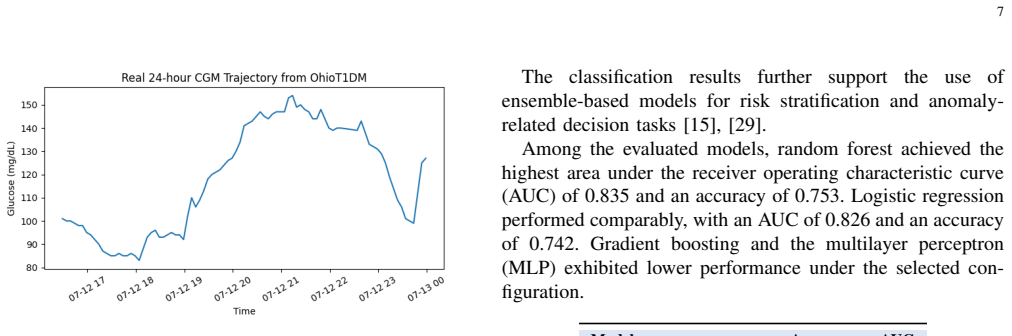
This paper presents a proof-of-concept digital twin framework for simulation-driven diabetes modeling using benchmark clinical data, synthetic temporal augmentation, and illustrative continuous glucose monitoring (CGM) analysis. Unlike traditional predictive models, the framework focuses on generating interpretable simulated trajectories rather than clinically validated outcomes. Evaluation is conducted using a public dataset combined with controlled synthetic scenarios to illustrate temporal behavior and intervention effects. Results illustrate the feasibility of integrating prediction with counterfactual simulation for decision-aware analysis. This work does not claim clinical readiness but provides a foundation for future research on simulation-driven digital twin systems in healthcare.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents a proof-of-concept simulation-driven digital twin framework for diabetes modeling. It combines public benchmark clinical data with controlled synthetic temporal augmentation to generate illustrative continuous glucose monitoring (CGM) trajectories, with the goal of integrating predictive modeling and counterfactual simulation to support decision-aware analysis. The work explicitly disclaims clinical validation or readiness and positions itself as a feasibility demonstration and foundation for future research.
Significance. If the synthetic trajectories can be shown to remain statistically representative of real patient CGM data, the framework could provide a useful simulation platform for exploring intervention effects without requiring new clinical trials. The current illustrative results, however, supply no quantitative support for this representativeness, limiting the work to a conceptual starting point rather than a substantive advance in digital-twin methodology for healthcare.
major comments (1)
- [Evaluation] Evaluation section (as described in the abstract and results): The central claim that the framework illustrates feasibility of decision-aware counterfactual analysis rests on the premise that benchmark data plus controlled synthetic temporal augmentation produces trajectories sufficiently representative for meaningful analysis. No quantitative fidelity metrics are supplied (e.g., preservation of glucose variability, autocorrelation structure, or time-in-range distributions) to confirm that the generated trajectories lie within the statistical envelope of real CGM data rather than reflecting artifacts of the augmentation rules.
minor comments (2)
- [Abstract] The abstract and introduction could more explicitly delineate the predictive model, the augmentation procedure, and the counterfactual generation steps so that readers can assess the integration claimed in the title.
- [Methods] A brief discussion of the specific public dataset employed and any preprocessing steps would improve reproducibility of the illustrative scenarios.
Simulated Author's Rebuttal
We thank the referee for their constructive feedback on our proof-of-concept manuscript. The evaluation concern is addressed point by point below.
read point-by-point responses
-
Referee: [Evaluation] Evaluation section (as described in the abstract and results): The central claim that the framework illustrates feasibility of decision-aware counterfactual analysis rests on the premise that benchmark data plus controlled synthetic temporal augmentation produces trajectories sufficiently representative for meaningful analysis. No quantitative fidelity metrics are supplied (e.g., preservation of glucose variability, autocorrelation structure, or time-in-range distributions) to confirm that the generated trajectories lie within the statistical envelope of real CGM data rather than reflecting artifacts of the augmentation rules.
Authors: We agree that the manuscript does not provide quantitative fidelity metrics to assess how well the synthetic trajectories preserve statistical properties of the benchmark CGM data. Given the explicit positioning of the work as a proof-of-concept feasibility demonstration (rather than a clinically validated system), the original focus was on illustrating the integration of benchmark data, controlled augmentation, and counterfactual simulation. However, we recognize that adding such metrics would strengthen the support for the framework's utility. In the revised manuscript, we will include quantitative comparisons of key CGM characteristics, such as glucose variability (standard deviation and coefficient of variation), time-in-range distributions, and autocorrelation structure, between the original benchmark data and the augmented trajectories. These additions will help demonstrate that the generated trajectories remain within a reasonable statistical envelope of real data. revision: yes
Circularity Check
No circularity; framework is self-contained using external public data and synthetic generation without derivations or self-referential fits.
full rationale
The paper is a proof-of-concept description of a digital twin framework that combines benchmark clinical data with controlled synthetic temporal augmentation to illustrate simulated trajectories and counterfactuals. No equations, parameter fittings, or derivation chains are present that would reduce any prediction or result to the inputs by construction. The work explicitly positions itself as non-clinically validated and illustrative, relying on existing public datasets rather than any self-citation load-bearing uniqueness theorems or ansatz smuggling. This matches the default expectation of a non-circular simulation study.
Axiom & Free-Parameter Ledger
Lean theorems connected to this paper
-
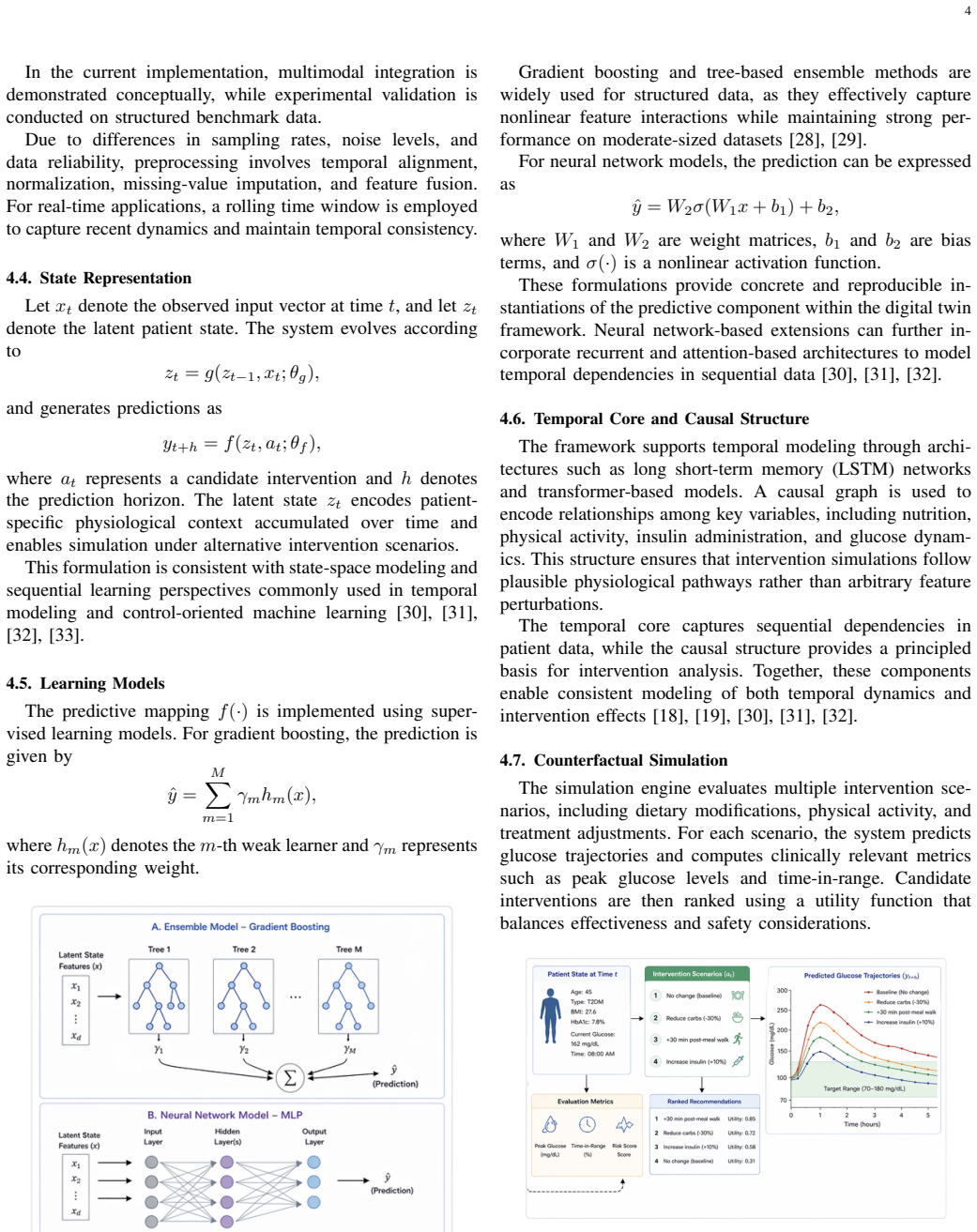
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel uncleargradient boosting regression... LSTM... transformer-based models... counterfactual simulation by perturbing carbohydrate intake, physical activity duration
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear8-tick period... 3 spatial dimensions... φ-powers on the recognition ladder
Reference graph
Works this paper leans on
-
[1]
Artificial intelligence for diabetes management and decision support: literature review,
I. Contreras and J. Vehí, “Artificial intelligence for diabetes management and decision support: literature review,”J. Diabetes Sci. Technol., vol. 12, no. 2, pp. 456–461, 2018
work page 2018
-
[2]
Machine learning and data mining methods in diabetes research,
I. Kavakiotis et al., “Machine learning and data mining methods in diabetes research,”Comput. Struct. Biotechnol. J., vol. 15, pp. 104–116, 2017
work page 2017
-
[3]
C. Ji, T. Jiang, L. Liu, J. Zhang, and L. You, “Continuous glucose monitoring combined with artificial intelligence: redefining the pathway for prediabetes management,”Frontiers in Endocrinology, vol. 16, Art. no. 1571362, 2025, doi: 10.3389/fendo.2025.1571362
-
[4]
Digital twins in Type 1 diabetes: A systematic review,
G. Cappon and A. Facchinetti, “Digital twins in Type 1 diabetes: A systematic review,”Journal of Diabetes Science and Technology, vol. 19, no. 6, pp. 1641–1649, Nov. 2025, doi: 10.1177/19322968241262112
-
[5]
Digital twins and artificial intelligence in metabolic disease research,
C. Mosquera-Lopez and P. G. Jacobs, “Digital twins and artificial intelligence in metabolic disease research,”Trends in Endocrinol- ogy & Metabolism, vol. 35, no. 6, pp. 549–557, Jun. 2024, doi: 10.1016/j.tem.2024.04.019
-
[6]
Digital twins in healthcare: a comprehensive review and future directions,
H. Khoshfekr Rudsari, B. Tseng, H. Zhu, L. Song, C. Gu, A. Roy, E. Irajizad, J. Butner, J. Long, and K.-A. Do, “Digital twins in healthcare: a comprehensive review and future directions,”Frontiers in Digital Health, vol. 7, Art. no. 1633539, 2025, doi: 10.3389/fdgth.2025.1633539
-
[7]
Digital twins in healthcare: Methodological challenges and opportunities,
C. Meijer, H.-W. Uh, and S. El Bouhaddani, “Digital twins in healthcare: Methodological challenges and opportunities,”Journal of Personalized Medicine, vol. 13, no. 10, Art. no. 1522, 2023, doi: 10.3390/jpm13101522
-
[8]
Personal- izing computational models to construct medical digital twins,
A. Knapp, D. A. Cruz, B. Mehrad, and R. C. Laubenbacher, “Personal- izing computational models to construct medical digital twins,”Journal of the Royal Society Interface, vol. 22, no. 228, Art. no. 20250055, Jul. 2025, doi: 10.1098/rsif.2025.0055
-
[9]
W. P. T. M. van Doorn, Y . D. Foreman, N. C. Schaper, H. H. C. M. Savel- berg, A. Koster, C. J. H. van der Kallen, A. Wesselius, M. T. Schram, R. M. A. Henry, P. C. Dagnelie, B. E. de Galan, O. Bekers, C. D. A. Stehouwer, S. J. R. Meex, and M. C. G. J. Brouwers, “Machine learning- based glucose prediction with use of continuous glucose and physical 10 act...
-
[10]
A hybrid Transformer-LSTM model apply to glucose prediction,
Q. Bian, A. As’arry, X. Cong, K. A. bin Md Rezali, and R. M. K. bin Raja Ahmad, “A hybrid Transformer-LSTM model apply to glucose prediction,”PLOS ONE, vol. 19, no. 9, Art. no. e0310084, Sep. 2024, doi: 10.1371/journal.pone.0310084
-
[11]
D. Darpit, K. Vyas, J. K. Jayagopal, A. Garcia, M. Erraguntla, and M. Lawley, “A personalized federated learning-based glucose predic- tion algorithm for high-risk glycemic excursion regions in Type 1 diabetes,”Scientific Reports, vol. 15, no. 1, Art. no. 38376, 2025, doi: 10.1038/s41598-025-22316-4
-
[12]
R. Alredaini, M. Abulkhair, and H. Almisbahi, “Interpretable glucose forecasting for Type 2 diabetes across traditional, deep, and large language models,”Scientific Reports, vol. 16, Art. no. 2421, 2025, doi: 10.1038/s41598-025-32373-4
-
[13]
D. Drummond and A. Coulet, “Technical, ethical, legal, and societal challenges with digital twin systems for the management of chronic diseases in children and young people,”Journal of Medical Internet Research, vol. 24, no. 10, Art. no. e39698, 2022, doi: 10.2196/39698
-
[14]
S. L. Cichosz, S. S. Olesen, and M. H. Jensen, “Explainable machine- learning models to predict weekly risk of hyperglycemia, hypo- glycemia, and glycemic variability in patients with Type 1 dia- betes based on continuous glucose monitoring,”Journal of Diabetes Science and Technology, vol. 20, no. 3, pp. 836–847, 2024, doi: 10.1177/19322968241286907
-
[15]
Z. Monirzadeh, M. Habibzadeh, and N. Farajian, “Detection of viola- tions in credit cards of banks and financial institutions based on artificial neural network and metaheuristic optimization algorithm,”International Journal of Advanced Computer Science and Applications, vol. 9, no. 1, pp. 176–182, 2018, doi: 10.14569/IJACSA.2018.090124
-
[16]
Available: https://doi.org/10.1038/s41591-018-0300-7
E. J. Topol, “High-performance medicine: the convergence of human and artificial intelligence,”Nature Medicine, vol. 25, no. 1, pp. 44–56, 2019, doi: 10.1038/s41591-018-0300-7
-
[17]
Scalable and accurate deep learning with electronic health records,
A. Rajkomar et al., “Scalable and accurate deep learning with electronic health records,”npj Digital Medicine, vol. 1, Art. no. 18, 2018, doi: 10.1038/s41746-018-0029-1
-
[18]
J. Pearl,Causality: Models, Reasoning, and Inference, 2nd ed. Cambridge, UK: Cambridge University Press, 2009, doi: 10.1017/CBO9780511803161
-
[19]
M. A. Hernán and J. M. Robins,Causal Inference: What If. Boca Raton, FL, USA: Chapman & Hall/CRC, 2020
work page 2020
-
[20]
The ‘digital twin’ to enable precision cardiol- ogy,
M. Corral-Acero et al., “The ‘digital twin’ to enable precision cardiol- ogy,”European Heart Journal, vol. 41, no. 48, pp. 4556–4564, 2020, doi: 10.1093/eurheartj/ehaa159
-
[21]
Digital twins in health care: ethical implications of an emerging engineering paradigm,
K. Bruynseels, F. Santoni de Sio, and J. van den Hoven, “Digital twins in health care: ethical implications of an emerging engineering paradigm,”Frontiers in Genetics, vol. 9, Art. no. 31, 2018, doi: 10.3389/fgene.2018.00031
-
[22]
In silico clinical trials: how computer simulation will transform the biomedical industry,
M. Viceconti, A. Henney, and E. Morley-Fletcher, “In silico clinical trials: how computer simulation will transform the biomedical industry,” Int. J. Clin. Trials, vol. 3, no. 2, pp. 37–46, 2016, doi: 10.18203/2349- 3259.ijct20161408
-
[23]
T. Zhu, K. Li, P. Herrero, and P. Georgiou, “Personalized blood glucose prediction for Type 1 diabetes using evidential deep learning and meta- learning,”IEEE Transactions on Biomedical Engineering, vol. 69, no. 10, pp. 3107–3118, 2022, doi: 10.1109/TBME.2022.3150729
-
[24]
Deep multi- output forecasting: learning to accurately predict blood glucose trajec- tories,
I. Fox, L. Ang, M. Jaiswal, R. Pop-Busui, and J. Wiens, “Deep multi- output forecasting: learning to accurately predict blood glucose trajec- tories,” inProc. 24th ACM SIGKDD Int. Conf. Knowl. Discovery Data Mining (KDD), 2018, pp. 1387–1395, doi: 10.1145/3219819.3220102
-
[25]
Dilated recurrent neural networks for glucose forecasting in Type 1 diabetes,
T. Zhu, K. Li, J. Chen, P. Herrero, and P. Georgiou, “Dilated recurrent neural networks for glucose forecasting in Type 1 diabetes,”Journal of Healthcare Engineering, vol. 2020, Art. no. 5847940, 2020, doi: 10.1155/2020/5847940
-
[26]
Digital twin for healthcare systems,
A. Vallée, “Digital twin for healthcare systems,”Frontiers in Digital Health, vol. 5, Art. no. 1253050, 2023, doi: 10.3389/fdgth.2023.1253050
-
[27]
Benchmarking deep learning models on large healthcare datasets,
S. Purushotham, C. Meng, Z. Che, and Y . Liu, “Benchmarking deep learning models on large healthcare datasets,”Journal of Biomedical Informatics, vol. 83, pp. 112–134, 2018, doi: 10.1016/j.jbi.2018.04.007
-
[28]
T. Chen and C. Guestrin, “XGBoost: A scalable tree boosting system,” inProc. 22nd ACM SIGKDD Int. Conf. Knowledge Discovery and Data Mining (KDD), San Francisco, CA, USA, 2016, pp. 785–794, doi: 10.1145/2939672.2939785
-
[29]
L. Breiman, “Random forests,”Machine Learning, vol. 45, no. 1, pp. 5–32, 2001, doi: 10.1023/A:1010933404324
-
[30]
Y . LeCun, Y . Bengio, and G. Hinton, “Deep learning,”Nature, vol. 521, no. 7553, pp. 436–444, 2015, doi: 10.1038/nature14539
-
[31]
S. Hochreiter and J. Schmidhuber, “Long short-term memory,” Neural Computation, vol. 9, no. 8, pp. 1735–1780, 1997, doi: 10.1162/neco.1997.9.8.1735
-
[32]
A. Vaswani, N. Shazeer, N. Parmar, J. Uszkoreit, L. Jones, A. N. Gomez, Ł. Kaiser, and I. Polosukhin, “Attention is all you need,” inProc. 31st Conf. Neural Information Processing Systems (NeurIPS), Long Beach, CA, USA, 2017, pp. 6000–6010
work page 2017
-
[33]
R. S. Sutton and A. G. Barto,Reinforcement Learning: An Introduction, 2nd ed. Cambridge, MA, USA: MIT Press, 2018
work page 2018
-
[34]
D. Silveret al., “Mastering the game of Go with deep neural networks and tree search,”Nature, vol. 529, no. 7587, pp. 484–489, 2016, doi: 10.1038/nature16961
-
[35]
A unified approach to interpreting model predictions,
S. M. Lundberg and S.-I. Lee, “A unified approach to interpreting model predictions,” inProc. 31st Conf. Neural Information Processing Systems (NeurIPS), Long Beach, CA, USA, 2017, pp. 4765–4774
work page 2017
-
[36]
M. T. Ribeiro, S. Singh, and C. Guestrin, “Why should I trust you?: Ex- plaining the predictions of any classifier,” inProc. 22nd ACM SIGKDD Int. Conf. Knowledge Discovery and Data Mining (KDD), San Francisco, CA, USA, 2016, pp. 1135–1144, doi: 10.1145/2939672.2939778
-
[37]
R. Caruana, Y . Lou, J. Gehrke, P. Koch, M. Sturm, and N. Elhadad, “In- telligible models for healthcare: Predicting pneumonia risk and hospital 30-day readmission,” inProc. 21st ACM SIGKDD Int. Conf. Knowledge Discovery and Data Mining (KDD), Sydney, NSW, Australia, 2015, pp. 1721–1730, doi: 10.1145/2783258.2788613
-
[38]
Deep learning: A critical appraisal,
G. Marcus, “Deep learning: A critical appraisal,” arXiv preprint arXiv:1801.00631, 2018, doi: 10.48550/arXiv.1801.00631
-
[39]
S. Waris, H. H. Begam, M. P. Kumar, Z. H. I. Abdulrasool, M. Avudaiappan, A. E. Butler, and M. Nandakumar, “Stem cell-derived beta-cell therapies: Encapsulation advances and immunological hurdles in diabetes treatment,”Cells, vol. 15, no. 2, Art. no. 191, 2026, doi: 10.3390/cells15020191
-
[40]
The OhioT1DM dataset for blood glucose level prediction: update 2020,
C. Marling and R. Bunescu, “The OhioT1DM dataset for blood glucose level prediction: update 2020,” inProc. 5th Int. Workshop Knowl. Discovery Healthcare Data (KDH), vol. 2675, pp. 71–74, 2020
work page 2020
-
[41]
A Proof-of-Concept Simulation-Driven Digital Twin Framework for Decision-Aware Diabetes Modeling,
Z. Monirzadeh, “A Proof-of-Concept Simulation-Driven Digital Twin Framework for Decision-Aware Diabetes Modeling,” GitHub repos- itory, 2026. [Online]. Available: https://github.com/zarrinmonirzadeh/ diabetes-ai-ml-digital-twin
work page 2026
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.