HoT-SSM:Higher-order Temporal Knowledge Graph Reasoning with State Space Models for Health Care
Pith reviewed 2026-06-28 02:57 UTC · model grok-4.3
The pith
HoT-SSM builds hypergraphs of related clinical concepts per visit and runs a dynamic state space model on them to track patient state changes across time.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
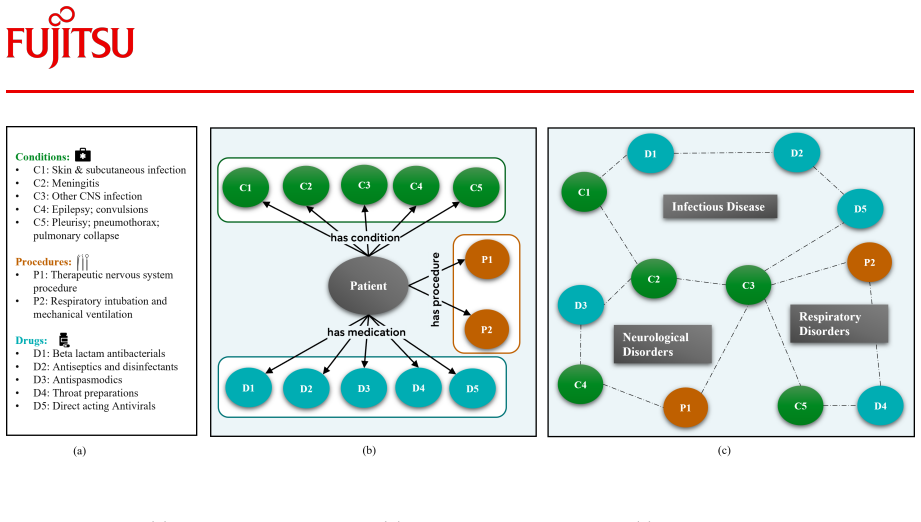
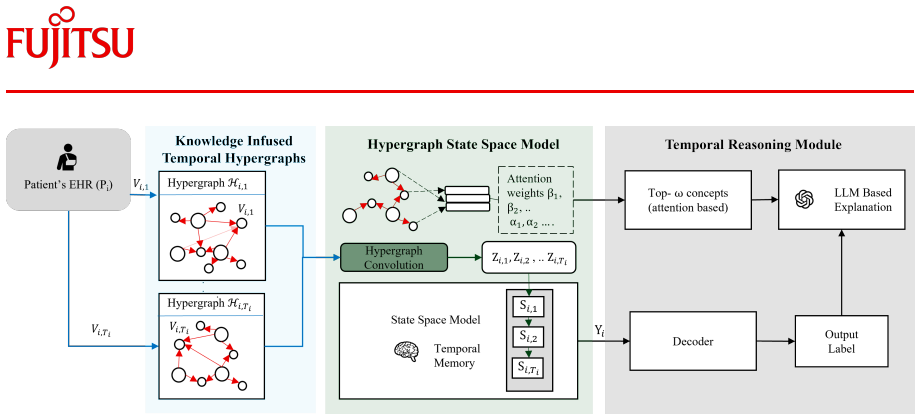
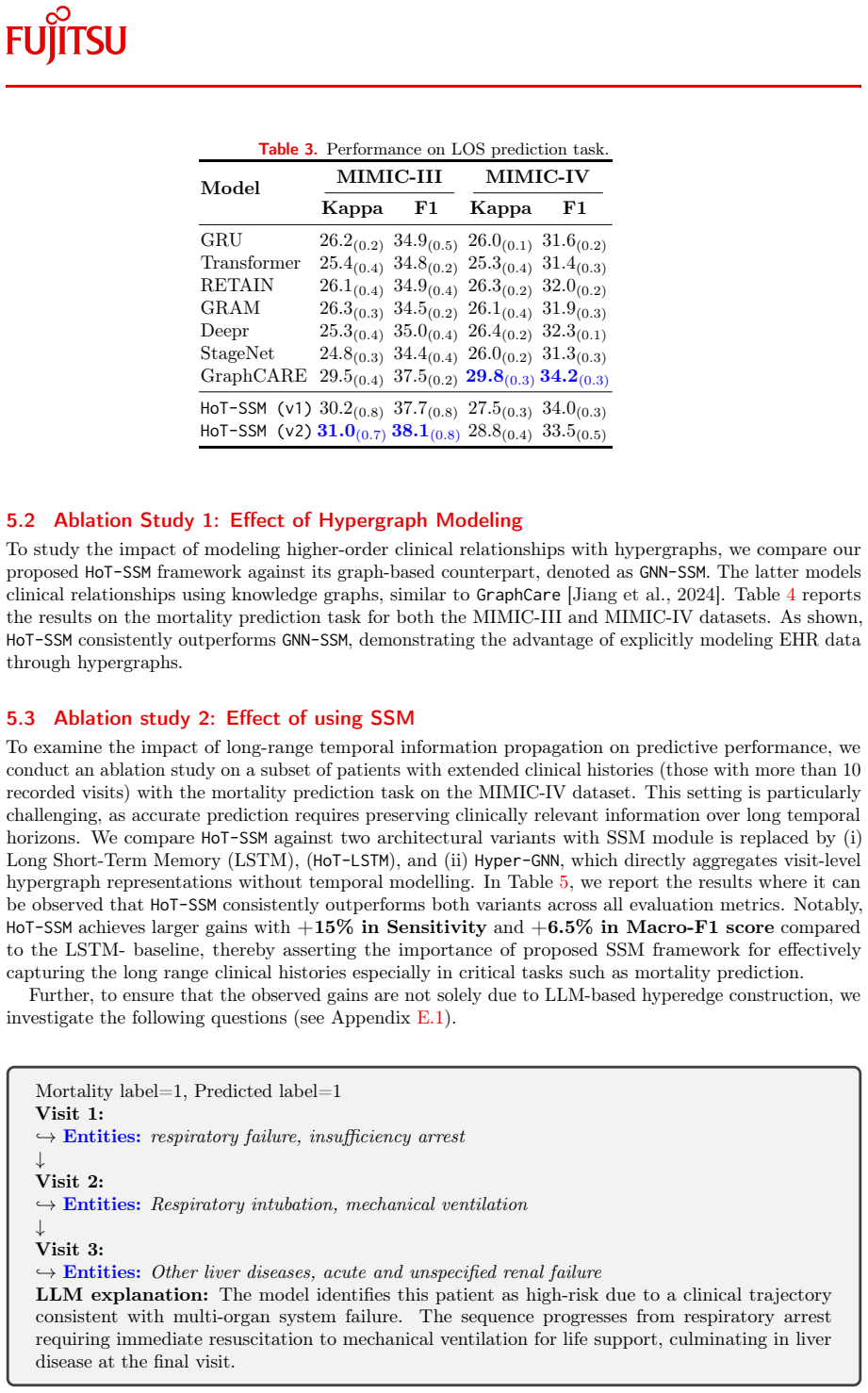
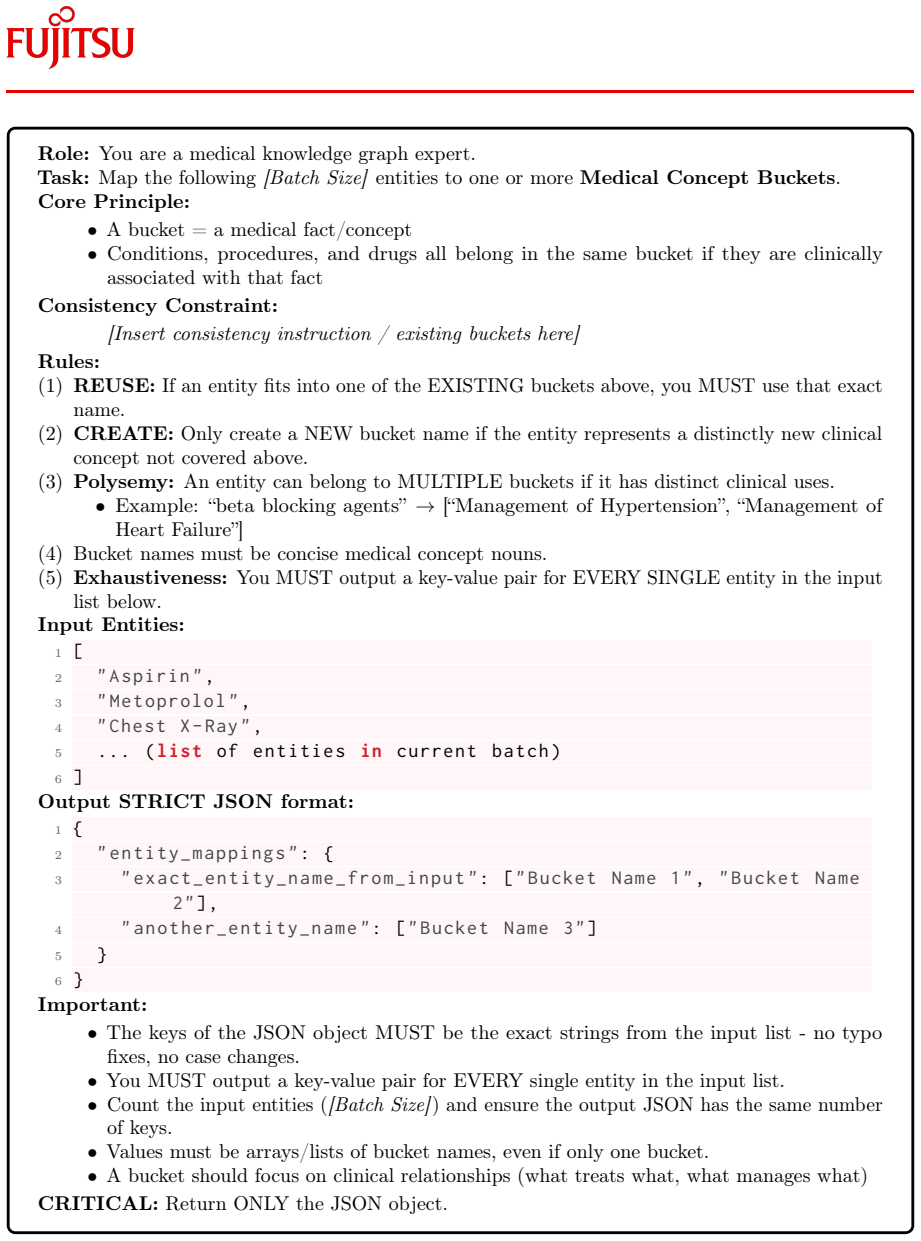
HoT-SSM constructs hypergraphs by grouping semantically related clinical concepts into hyperedges for each visit using domain knowledge, thereby preserving visit-level clinical context. It then applies a novel dynamic hypergraph-based state space model that explicitly captures patients' latent state evolution over time while preserving long-range information. The learned representations support downstream clinical prediction and reasoning, with experiments on MIMIC-III and MIMIC-IV showing significant gains over current state-of-the-art models.
What carries the argument
Dynamic hypergraph-based state space model that converts per-visit hypergraphs of clinical concepts into sequential state updates.
If this is right
- Clinical predictions such as mortality can improve by jointly handling higher-order concept interactions and long-range visit sequences rather than pairwise or collapsed representations.
- Visit-level context remains explicit because hyperedges keep co-occurring or related concepts together instead of flattening them into pairs.
- Parameter-efficient training becomes feasible because the state space model processes the hypergraph sequence without quadratic attention costs over long histories.
- The same learned representations support multiple downstream reasoning tasks on the same patient timeline.
Where Pith is reading between the lines
- The reliance on domain knowledge for hyperedge creation could be relaxed by learning the grouping rules from data, potentially allowing the method to adapt to new medical domains with less expert input.
- Because the state space model maintains an explicit latent state, the approach may lend itself to counterfactual queries about how a change in one visit would propagate through later states.
- The architecture could be tested on non-medical sequential relational data, such as user-item interaction logs or sensor networks, to check whether the hypergraph-plus-state-space combination transfers.
Load-bearing premise
Grouping semantically related clinical concepts into hyperedges with domain knowledge preserves the true visit-level context and lets the state space model track latent patient state evolution without losing long-range temporal signals.
What would settle it
A controlled ablation on MIMIC-III or MIMIC-IV in which either the hyperedge grouping step or the state space temporal component is removed and performance returns to the level of prior pairwise or short-range baselines.
Figures




read the original abstract
Medical knowledge graphs (MKGs) infused with clinical knowledge have been increasingly used to model electronic health records (EHRs) to support interpretable predictions in healthcare domain. However, existing MKG-based approaches are limited in capturing pairwise relations between clinical concepts (e.g., conditions, procedures, and medications), and restricts their ability to model higher-order interactions among co-occurring or semantically related concepts. In addition, most representation learning methods that leverage MKGs either collapse temporal information across visits or lack an explicit mechanism for modeling long-range temporal dependencies, which is critical for clinical tasks such as mortality prediction. To mitigate these limitations, we propose HoT-SSM, a parameter efficient and higher-order temporal graph reasoning with state space models. For each visit, HoT-SSM constructs hypergraphs by grouping semantically related clinical concepts into hyperedges using domain knowledge, thereby preserving visit-level clinical context. Further, to model the temporal dynamics while learning the representations, we introduce a novel dynamic hypergraph-based state space model that explicitly captures patients latent state evolution over time while preserving long-range information. The learned representations are used for downstream clinical prediction and reasoning. Experiments on MIMIC-III and MIMIC-IV datasets shows significant performance improvement over the current state-of-the-art models, demonstrating the effectiveness of jointly modeling higher-order clinical interactions and long-range temporal dependencies.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes HoT-SSM, a parameter-efficient model for higher-order temporal knowledge graph reasoning in healthcare. For each patient visit, it constructs hypergraphs by grouping semantically related clinical concepts (conditions, procedures, medications) into hyperedges using domain knowledge. It then applies a novel dynamic hypergraph-based state space model to capture patients' latent state evolution over time while preserving long-range temporal dependencies. The learned representations support downstream tasks such as mortality prediction. Experiments on MIMIC-III and MIMIC-IV are reported to show significant improvements over state-of-the-art models, attributing gains to the joint modeling of higher-order interactions and temporal dynamics.
Significance. If the central claims hold after validation, the work could meaningfully extend MKG-based EHR modeling beyond pairwise relations and collapsed temporal information, offering a more expressive way to handle co-occurring clinical concepts and long-range patient trajectories. The parameter-efficient SSM adaptation and domain-knowledge hyperedges are potentially reusable ideas for other temporal graph tasks in medicine.
major comments (4)
- [Abstract, §3] Abstract and §3 (model description): the headline claim of 'significant performance improvement' and 'effectiveness of jointly modeling higher-order clinical interactions and long-range temporal dependencies' is not accompanied by any quantitative results, baseline comparisons, or ablation tables in the provided abstract; without these, the data cannot be checked against the claim.
- [§3.1] §3.1 (hypergraph construction): the assumption that grouping semantically related concepts into hyperedges via domain knowledge 'preserves visit-level clinical context' without loss or spurious aggregation lacks any ablation isolating domain-knowledge hyperedges versus random hyperedges or standard pairwise edges; this is load-bearing for the higher-order interaction claim.
- [§3.2] §3.2 (dynamic hypergraph SSM): no derivation or explicit recurrence is shown for extending standard SSM state transitions to hypergraph signals; it is unclear how the model retains higher-order structure rather than collapsing to pairwise or node-level updates, undermining the 'explicitly captures patients latent state evolution' claim.
- [Experiments] Experiments section: the reported gains on MIMIC-III/IV are attributed to the joint higher-order + temporal mechanism, yet no ablation or sensitivity analysis tests whether the gains persist when the hypergraph component is replaced by a standard graph SSM or when domain knowledge is removed.
minor comments (2)
- [§3] Notation for hyperedge construction and SSM parameters should be defined explicitly with equations rather than prose descriptions.
- [Abstract] The abstract states results without any numbers, baselines, or dataset statistics; this should be expanded to include at least key metrics and model sizes.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive feedback. We agree that the manuscript would benefit from additional quantitative support in the abstract, explicit derivations, and targeted ablations. Below we respond point-by-point and commit to revisions that directly address each concern while preserving the core technical contributions.
read point-by-point responses
-
Referee: [Abstract, §3] Abstract and §3 (model description): the headline claim of 'significant performance improvement' and 'effectiveness of jointly modeling higher-order clinical interactions and long-range temporal dependencies' is not accompanied by any quantitative results, baseline comparisons, or ablation tables in the provided abstract; without these, the data cannot be checked against the claim.
Authors: We accept this observation. The original abstract summarized results qualitatively. In the revision we will insert the key quantitative results (e.g., AUC-ROC and AUPRC deltas versus the strongest baselines on both MIMIC-III and MIMIC-IV) directly into the abstract so that the headline claims are immediately verifiable. revision: yes
-
Referee: [§3.1] §3.1 (hypergraph construction): the assumption that grouping semantically related concepts into hyperedges via domain knowledge 'preserves visit-level clinical context' without loss or spurious aggregation lacks any ablation isolating domain-knowledge hyperedges versus random hyperedges or standard pairwise edges; this is load-bearing for the higher-order interaction claim.
Authors: The construction relies on established clinical ontologies to form hyperedges; however, we did not provide an explicit ablation against random hyperedges or pairwise graphs. We will add this ablation (domain-knowledge hyperedges vs. random hyperedges vs. standard pairwise edges) to §4, reporting the resulting performance drop to quantify the value of the domain-knowledge step. revision: yes
-
Referee: [§3.2] §3.2 (dynamic hypergraph SSM): no derivation or explicit recurrence is shown for extending standard SSM state transitions to hypergraph signals; it is unclear how the model retains higher-order structure rather than collapsing to pairwise or node-level updates, undermining the 'explicitly captures patients latent state evolution' claim.
Authors: Section 3.2 presents the high-level architecture but omits the full recurrence. We will insert a concise derivation of the hypergraph-aware state transition (showing how the selective SSM operates on hyperedge embeddings and how the output is projected back to nodes without reducing to pairwise operations) together with the explicit recurrence equations. revision: yes
-
Referee: [Experiments] Experiments section: the reported gains on MIMIC-III/IV are attributed to the joint higher-order + temporal mechanism, yet no ablation or sensitivity analysis tests whether the gains persist when the hypergraph component is replaced by a standard graph SSM or when domain knowledge is removed.
Authors: We will expand the experimental section with two additional ablation tables: (1) HoT-SSM versus a graph-SSM variant that replaces hyperedges with ordinary edges, and (2) domain-knowledge hyperedges versus randomly generated hyperedges of the same cardinality. These results will isolate the contribution of each design choice. revision: yes
Circularity Check
No circularity; derivation chain is self-contained with external experimental validation
full rationale
The paper describes a modeling approach using domain-knowledge hyperedges and a dynamic hypergraph SSM but presents no equations, derivations, or fitted-parameter predictions in the abstract or visible text. Claims rest on experimental results on external MIMIC-III/IV benchmarks rather than any reduction of outputs to inputs by construction. No self-citations, uniqueness theorems, or ansatzes are invoked in a load-bearing way. The central performance gains are attributed to the proposed architecture without evidence of statistical forcing or renaming of known results.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption Domain knowledge can be used to group semantically related clinical concepts into hyperedges that preserve visit-level context.
- domain assumption A dynamic hypergraph-based state space model can capture latent state evolution while preserving long-range temporal information.
Reference graph
Works this paper leans on
-
[1]
Junde Wu, Jiayuan Zhu, Yunli Qi, Jingkun Chen, Min Xu, Filippo Menolascina, and Vicente Grau. Medical graph rag: Towards safe medical large language model via graph retrieval-augmented generation. arXiv preprint arXiv:2408.04187,
-
[2]
Applying personal knowledge graphs to health.arXiv preprint arXiv:2104.07587,
Sola Shirai, Oshani Seneviratne, and Deborah L McGuinness. Applying personal knowledge graphs to health.arXiv preprint arXiv:2104.07587,
-
[3]
BERT: Pre-training of Deep Bidirectional Transformers for Language Understanding
URLhttps://arxiv.org/abs/1810.04805. Song Bai, Feihu Zhang, and Philip HS Torr. Hypergraph convolution and hypergraph attention.Pattern Recognition, 110:107637,
work page internal anchor Pith review Pith/arXiv arXiv
-
[4]
Be more with less: Hypergraph attention networks for inductive text classification
Kaize Ding, Jianling Wang, Jundong Li, Dingcheng Li, and Huan Liu. Be more with less: Hypergraph attention networks for inductive text classification. InProceedings of the 2020 Conference on Empirical Methods in Natural Language Processing (EMNLP), pages 4927–4936,
2020
-
[5]
Stagenet: Stage-aware neural networks for health risk prediction
Junyi Gao, Cao Xiao, Yasha Wang, Wen Tang, Lucas M Glass, and Jimeng Sun. Stagenet: Stage-aware neural networks for health risk prediction. InProceedings of the web conference 2020, pages 530–540,
2020
-
[6]
Negin Ashrafi, Armin Abdollahi, Jiahong Zhang, and Maryam Pishgar. Optimizing mortality prediction for icu heart failure patients: Leveraging xgboost and advanced machine learning with the mimic-iii database.arXiv preprint arXiv:2409.01685,
-
[7]
Empirical Evaluation of Gated Recurrent Neural Networks on Sequence Modeling
Junyoung Chung, Caglar Gulcehre, KyungHyun Cho, and Yoshua Bengio. Empirical evaluation of gated recurrent neural networks on sequence modeling.arXiv preprint arXiv:1412.3555,
work page internal anchor Pith review Pith/arXiv arXiv
-
[8]
Molerec: Combinatorial drug recommendation with substructure-aware molecular representation learning
Nianzu Yang, Kaipeng Zeng, Qitian Wu, and Junchi Yan. Molerec: Combinatorial drug recommendation with substructure-aware molecular representation learning. InProceedings of the ACM web conference 2023, pages 4075–4085,
2023
-
[9]
Hypergraph transformers for ehr-based clinical predictions.AMIA Summits on Translational Science Proceedings, 2023:582,
Ran Xu, Mohammed K Ali, Joyce C Ho, and Carl Yang. Hypergraph transformers for ehr-based clinical predictions.AMIA Summits on Translational Science Proceedings, 2023:582,
2023
-
[10]
doi: 10.1109/JBHI.2016.2633963. 11 APPENDIX (1) Prior Works ................................................................................12 (2) Proof of Theorems ..........................................................................12 (3) Implementation Details .....................................................................15 (4) Dataset and ...
-
[11]
denotes the canonical basis vectors
Further, if we impose structure on the perturbation-specifically modeling it as arising from hyperedge addition or deletion-the perturbed hypergraph Laplacian can be written in the formˆL =L+ ρP j bjb⊤ j , where ρ∈ { +1,− 1} corresponds to edge addition or deletion, respectively, andbj ∈R N×1 is an incidence vector with entries as+1at one end point node a...
2020
-
[12]
• Taxonomy (Phase 1): We first induce a global medical taxonomy by processing a representative subset of the corpus
Global HyperKnowledge Graph Construction: To ensure semantic consistency across the EHR dataset, we create global hyperknowledge graph in two phases inspired by TnT-LLM architecture [Wan et al., 2024]. • Taxonomy (Phase 1): We first induce a global medical taxonomy by processing a representative subset of the corpus. This stage corresponds to the taxonomy...
2024
-
[13]
metoprolol
15 Table 6.Examples of global hyperedges constructed during the taxonomy discovery phase. Example Global Hyperedges Gastrointestinal Disease Heart Failure Example entities: Example entities: • Agents for treatment of hemorhoids and anal fissures (topical) •Antacids •Antidiarrheal microorganisms •Gastritis and duodenitis •Nausea and vomiting •Gastrointesti...
2016
-
[14]
The results show that the proposed model consistently outperforms existing approaches, highlighting the importance of jointly modeling higher-order relationships
Table 16.Performance comparison on readmission prediction task Task: Readmission Prediction Model MIMIC-III MIMIC-IV AUPRC AUROC AUPRC AUROC GRU 68.2 (0.4) 65.4(0.8) 66.1(0.7) 66.2(0.1) Transformer 67.3 (0.7) 63.9(1.1) 65.7(0.3) 65.3(0.4) RETAIN 65.1 (1.0) 64.1(0.7) 66.2(0.3) 65.3(0.2) GRAM 67.2 (0.8) 64.3(0.4) 66.1(0.2) 66.3(0.3) Deepr 68.8 (0.9) 66.5(0....
2023
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.