Sequence models reveal diagnosis accumulation pathways beyond comorbidity burden in population-scale hospital data
Pith reviewed 2026-06-28 20:13 UTC · model grok-4.3
The pith
Longitudinal hospital diagnosis sequences contain predictive information beyond age, sex, and comorbidity burden.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
A visit-level contrastive transformer encodes diagnosis sequences and inter-admission timing into patient-history embeddings that improve prediction of 93 of 131 incident ICD-10 disease blocks over Elixhauser-based models, with the added signal concentrated in the breadth, recency, and pace of prior disease accumulation as measured by reduced event-free survival.
What carries the argument
visit-level contrastive transformer that encodes diagnosis sequences and inter-admission timing into patient-history embeddings
If this is right
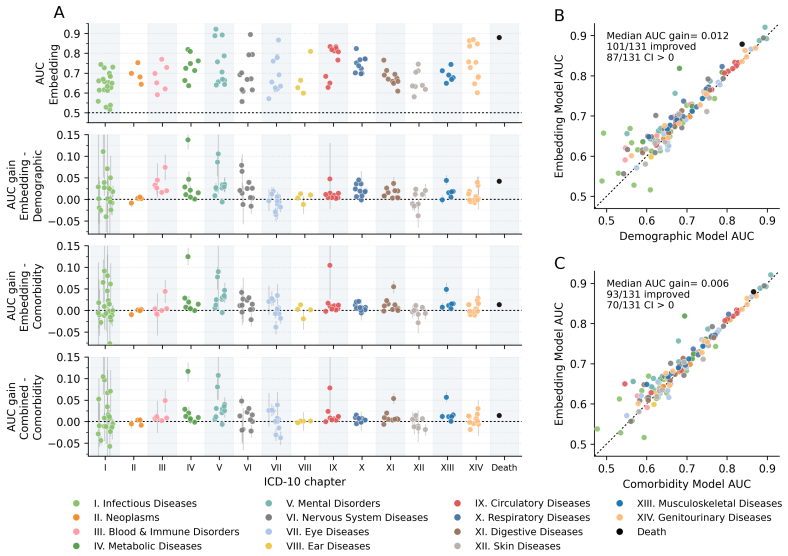
- Embeddings improve prediction for 93 of 131 incident disease blocks with a median AUC gain of 0.006.
- Gains concentrate in mental, musculoskeletal, nervous system, and metabolic disorders.
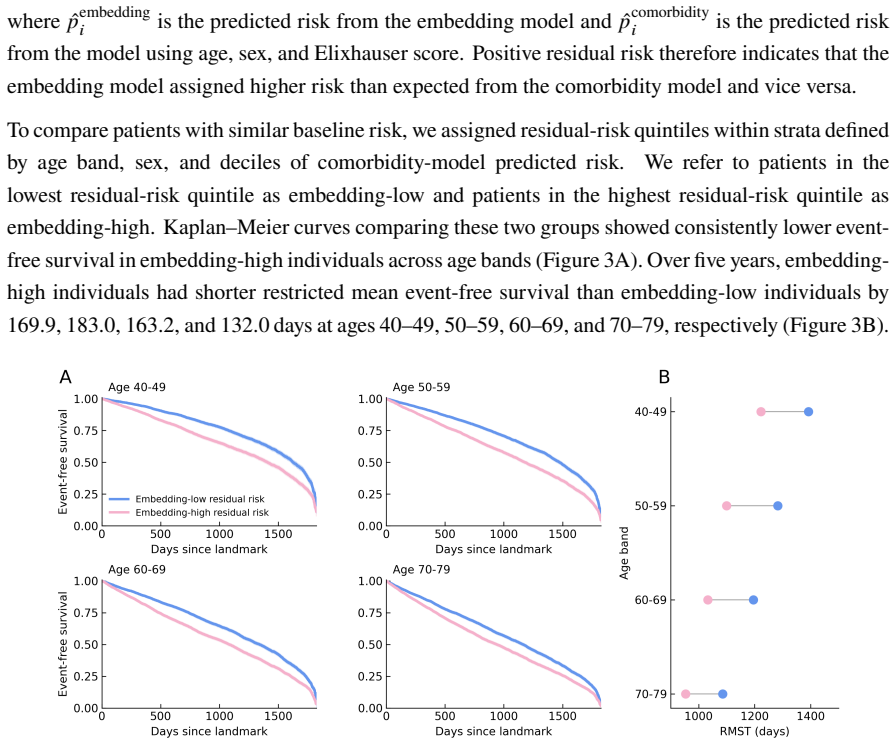
- Patients with high residual risk have 132-183 fewer event-free days over five years.
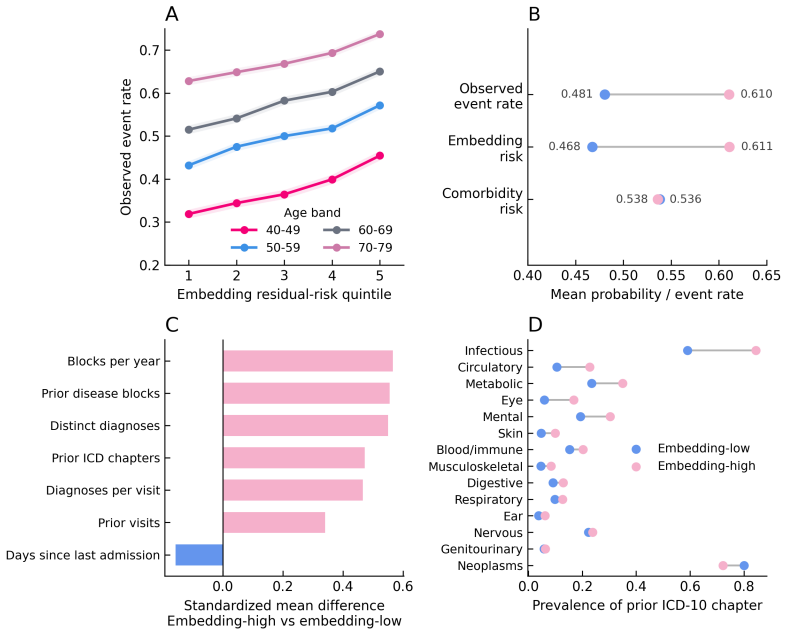
- Event rates for high-residual-risk patients match those of low-residual-risk patients more than a decade older.
- The embedding signal tracks the breadth, recency, and pace of prior disease accumulation.
Where Pith is reading between the lines
- The approach could be applied to outpatient or claims data to test whether sequence effects persist outside inpatient settings.
- Residual risk scores derived from embeddings might support targeted monitoring for patients showing rapid accumulation patterns.
- Shuffling diagnosis order in retraining experiments would isolate the contribution of sequence versus simple count of conditions.
- Similar embeddings could be compared across countries to examine whether accumulation pace varies by healthcare system.
Load-bearing premise
The embeddings from the contrastive transformer capture information about diagnosis sequences and timing that is not already contained in age, sex, and the Elixhauser comorbidity index.
What would settle it
A model that adds the embeddings to a baseline already containing the Elixhauser index, age, and sex shows no AUC improvement, or randomizing the order of diagnoses within patient histories removes the observed gains.
Figures
read the original abstract
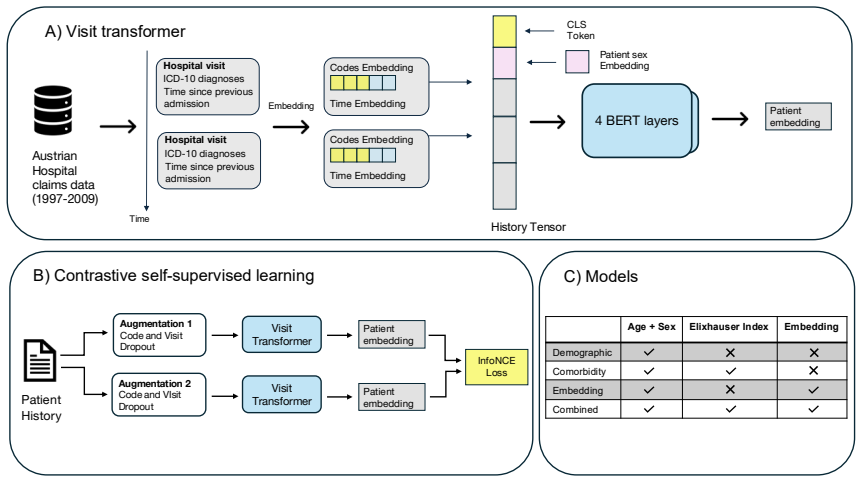
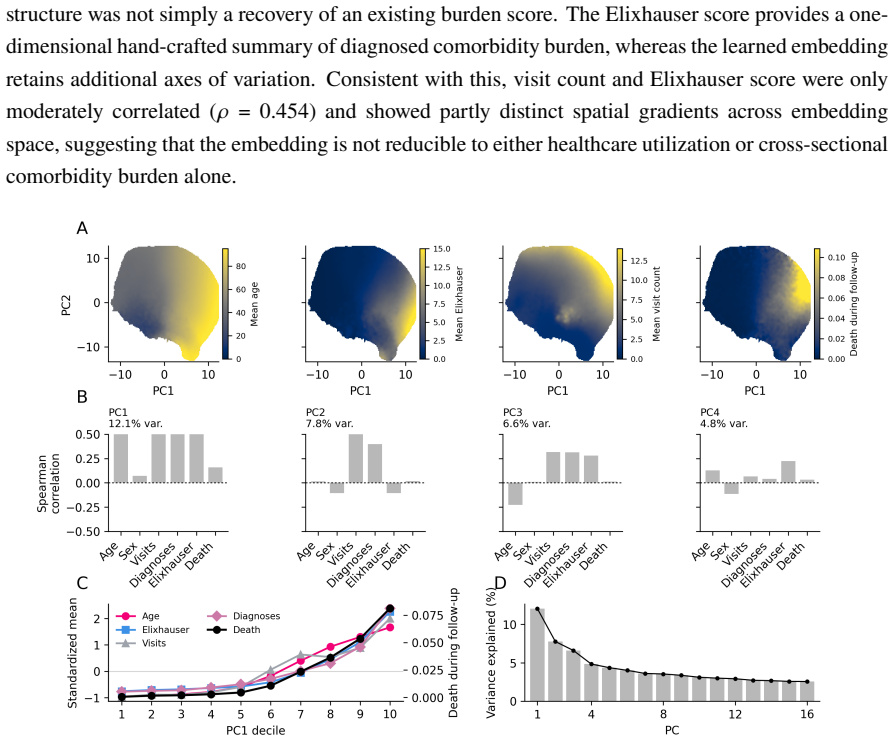
Aging trajectories vary among individuals of similar age and disease burden. Comorbidity indices, e.g. the Elixhauser index, summarize conditions cross-sectionally, but discard the timing, sequence, and pace of morbidity accumulation. Here we ask whether longitudinal hospital diagnosis histories contain information beyond age, sex, and comorbidity burden, and where it is concentrated. Using 13 years of Austrian inpatient data covering 7.4 million patients, we trained a visit-level contrastive transformer to encode diagnosis sequences and inter-admission timing into patient-history embeddings. In a downstream cohort of 1.7 million individuals, embeddings improved prediction over the Elixhauser-based comorbidity model for 93 of 131 incident ICD-10 disease-block outcomes, with a modest median AUC gain of 0.006. Gains concentrated in mental, musculoskeletal, nervous system, and metabolic disorders. We then evaluated event-free survival, defined as remaining alive without accumulating a second unrecorded ICD-10 disease block. The embedding model achieved an AUC of 0.726 versus 0.722 for the comorbidity model. However, among patients with similar age, sex, and comorbidity-model risk, those assigned high residual risk had 132--183 fewer event-free days over five years and observed event rates comparable to low-residual-risk patients more than a decade older. Together, these findings link the embedding's signal to the breadth, recency, and pace of prior disease accumulation.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper trains a visit-level contrastive transformer on 13 years of Austrian inpatient records (7.4M patients) to produce patient-history embeddings from diagnosis sequences and inter-admission intervals. These embeddings are evaluated in a 1.7M-patient downstream cohort and reported to improve prediction of 93/131 incident ICD-10 disease-block outcomes over an Elixhauser comorbidity baseline (median AUC gain 0.006), with additional gains in event-free survival (AUC 0.726 vs 0.722) that are linked to the breadth, recency, and pace of prior morbidity accumulation.
Significance. If the residual predictive signal is shown to originate from temporal ordering and timing rather than richer cross-sectional encoding of the same diagnoses, the result would demonstrate that sequence models can extract prognostic information beyond standard comorbidity indices in large-scale hospital data. The modest effect sizes and concentration in specific disease categories (mental, musculoskeletal, nervous, metabolic) limit immediate clinical translation but could inform targeted longitudinal risk modeling.
major comments (2)
- [Abstract] Abstract and implied Methods: the central claim that embeddings capture information 'beyond' the Elixhauser index requires an ablation that replaces the sequential contrastive transformer with a permutation-invariant aggregator (e.g., mean-pooled diagnosis embeddings or set transformer). Without this control, the reported median AUC lift of 0.006 cannot be attributed to sequence or timing rather than higher-capacity encoding of the identical past diagnoses.
- [Abstract] Abstract/Results: the modest median AUC gain (0.006) and survival AUC lift (0.004) are presented without reported confidence intervals, statistical tests for improvement, or assessment of calibration; given the sample size of 1.7M, even small gains may be statistically detectable yet clinically marginal, weakening the link to 'breadth, recency, and pace'.
minor comments (2)
- Clarify how inter-admission timing is tokenized and whether the contrastive objective explicitly penalizes or rewards temporal order.
- Specify the exact train/validation split between the embedding pre-training cohort and the 1.7M downstream cohort to rule out leakage.
Simulated Author's Rebuttal
We thank the referee for their thoughtful review and constructive feedback. We address the major comments point-by-point below.
read point-by-point responses
-
Referee: [Abstract] Abstract and implied Methods: the central claim that embeddings capture information 'beyond' the Elixhauser index requires an ablation that replaces the sequential contrastive transformer with a permutation-invariant aggregator (e.g., mean-pooled diagnosis embeddings or set transformer). Without this control, the reported median AUC lift of 0.006 cannot be attributed to sequence or timing rather than higher-capacity encoding of the identical past diagnoses.
Authors: We agree that demonstrating the specific contribution of sequential information requires an ablation against a permutation-invariant baseline. In the revised version, we will add this control experiment using mean-pooled embeddings of the same diagnosis representations, allowing direct comparison to isolate the effect of ordering and timing. revision: yes
-
Referee: [Abstract] Abstract/Results: the modest median AUC gain (0.006) and survival AUC lift (0.004) are presented without reported confidence intervals, statistical tests for improvement, or assessment of calibration; given the sample size of 1.7M, even small gains may be statistically detectable yet clinically marginal, weakening the link to 'breadth, recency, and pace'.
Authors: We will include bootstrap-derived confidence intervals for the AUC values and differences, along with p-values from appropriate statistical tests (e.g., DeLong's test for AUC comparison). We will also add calibration metrics and plots to the revised manuscript to provide a more complete evaluation of the model's performance. revision: yes
Circularity Check
No circularity: embeddings trained contrastively on sequences, evaluated on held-out downstream prediction against fixed external baseline
full rationale
The paper trains a visit-level contrastive transformer on diagnosis sequences and inter-admission timing to produce embeddings, then evaluates those embeddings as features for predicting incident disease blocks and event-free survival in a downstream cohort, reporting modest AUC gains over a fixed Elixhauser comorbidity model plus demographics. No step reduces by the paper's own equations or definitions to a quantity already fitted in the baseline; the contrastive objective operates on sequence order and timing, the baseline is an external non-learned index, and the prediction tasks are on held-out future outcomes. No self-citation chains, ansatzes smuggled via prior work, or fitted parameters renamed as predictions are present in the provided text. The derivation chain is therefore self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Contrastive learning on diagnosis sequences produces embeddings that capture temporal structure beyond cross-sectional counts
Reference graph
Works this paper leans on
-
[1]
Luigi Ferrucci and George A. Kuchel. Heterogeneity of Aging: Individual Risk Factors, Mech- anisms, Patient Priorities, and Outcomes.Journal of the American Geriatrics Society, 69 (3):610–612, March 2021. ISSN 0002-8614, 1532-5415. doi: 10.1111/jgs.17011. URL https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.17011
-
[2]
Moodie, Marie-France Forget, Philippe Desmarais, Mark R
Quoc Dinh Nguyen, Erica M. Moodie, Marie-France Forget, Philippe Desmarais, Mark R. Keezer, and Christina Wolfson. Health Heterogeneity in Older Adults: Exploration in the Canadian Longitudinal Study on Aging.Journal of the American Geriatrics Society, 69(3): 678–687, March 2021. ISSN 0002-8614, 1532-5415. doi: 10.1111/jgs.16919. URLhttps: //agsjournals.o...
-
[3]
Amaia Calderón-Larrañaga, Xiaonan Hu, Miriam Haaksma, Debora Rizzuto, Laura Fratiglioni, and Davide L. Vetrano. Health trajectories after age 60: the role of individual behaviors and the social context.Aging, 13(15):19186–19206, August 2021. ISSN 1945-4589. doi: 10.18632/agi ng.203407. URLhttps://www.aging-us.com/lookup/doi/10.18632/aging.203407
-
[4]
Siebra, Mascha Kurpicz-Briki, and Katarzyna Wac
Clauirton A. Siebra, Mascha Kurpicz-Briki, and Katarzyna Wac. Transformers in health: a systematic review on architectures for longitudinal data analysis.Artificial Intelligence Review, 57(2):32, February 2024. ISSN 1573-7462. doi: 10.1007/s10462-023-10677-z. URL https://link.springer.com/10.1007/s10462-023-10677-z
-
[5]
BEHRT: Transformer for Electronic Health Records.Scientific Reports, 10(1):7155, April 2020
Yikuan Li, Shishir Rao, José Roberto Ayala Solares, Abdelaali Hassaine, Rema Ramakrish- nan, Dexter Canoy, Yajie Zhu, Kazem Rahimi, and Gholamreza Salimi-Khorshidi. BEHRT: Transformer for Electronic Health Records.Scientific Reports, 10(1):7155, April 2020. ISSN 2045-2322. doi: 10.1038/s41598-020-62922-y. URLhttps://www.nature.com/article s/s41598-020-62922-y
-
[6]
ClinicalBERT: Modeling Clinical Notes and Predicting Hospital Readmission
Kexin Huang, Jaan Altosaar, and Rajesh Ranganath. ClinicalBERT: Modeling Clinical Notes and Predicting Hospital Readmission, November 2020. URLhttp://arxiv.org/abs/1904 .05342. arXiv:1904.05342 [cs]
work page internal anchor Pith review Pith/arXiv arXiv 2020
-
[7]
Laila Rasmy, Yang Xiang, Ziqian Xie, Cui Tao, and Degui Zhi. Med-BERT: pretrained contex- tualized embeddings on large-scale structured electronic health records for disease prediction. npjDigitalMedicine,4(1):86,May2021. ISSN2398-6352. doi: 10.1038/s41746-021-00455-y. URLhttps://www.nature.com/articles/s41746-021-00455-y
-
[8]
Yikuan Li, Mohammad Mamouei, Gholamreza Salimi-Khorshidi, Shishir Rao, Abdelaali Has- saine, Dexter Canoy, Thomas Lukasiewicz, and Kazem Rahimi. Hi-BEHRT: Hierarchical Transformer-Based Model for Accurate Prediction of Clinical Events Using Multimodal Longi- tudinal Electronic Health Records.IEEE Journal of Biomedical and Health Informatics, 27(2): 1106–1...
-
[9]
Zeljko Kraljevic, Dan Bean, Anthony Shek, Rebecca Bendayan, Harry Hemingway, Joshua Au Yeung, Alexander Deng, Alfred Balston, Jack Ross, Esther Idowu, James T Teo, and Richard J B Dobson. Foresight—a generative pretrained transformer for modelling of patient timelines using electronic health records: a retrospective modelling study.The Lancet Digital Heal...
-
[10]
Zhichao Yang, Avijit Mitra, Weisong Liu, Dan Berlowitz, and Hong Yu. TransformEHR: transformer-based encoder-decoder generative model to enhance prediction of disease outcomes using electronic health records.Nature Communications, 14(1):7857, November 2023. ISSN 22 2041-1723. doi: 10.1038/s41467-023-43715-z. URLhttps://www.nature.com/article s/s41467-023-43715-z
-
[11]
Hans Moen, Vishnu Raj, Andrius Vabalas, Markus Perola, Samuel Kaski, Andrea Ganna, and PekkaMarttinen. Towardsmodelingevolvinglongitudinalhealthtrajectorieswithatransformer- based deep learning model.Annals of Epidemiology, 111:30–43, November 2025. ISSN 10472797. doi: 10.1016/j.annepidem.2025.08.025. URLhttps://linkinghub.elsev ier.com/retrieve/pii/S1047...
-
[12]
Norah Hamad Alhumaidi, Doni Dermawan, Hanin Farhana Kamaruzaman, and Nasser Alotaiq. TheUseofMachineLearningforAnalyzingReal-WorldDatainDiseasePredictionandManage- ment: Systematic Review.JMIR Medical Informatics, 13:e68898, June 2025. ISSN 2291-9694. doi: 10.2196/68898. URLhttps://medinform.jmir.org/2025/1/e68898
-
[13]
Germans Savcisens, Tina Eliassi-Rad, Lars Kai Hansen, Laust Hvas Mortensen, Lau Lilleholt, Anna Rogers, Ingo Zettler, and Sune Lehmann. Using sequences of life-events to predict human lives.Nature Computational Science, 4(1):43–56, January 2024. ISSN 2662-8457. doi: 10.1038/s43588-023-00573-5. URLhttps://doi.org/10.1038/s43588-023-00573-5
-
[14]
SurvivEHR: a competing risks, time-to-event foundation model for multiple long-term conditions from primary care electronic health records
Charles Gadd, Krishna Gokhale, Aditya Acharya, Jennifer Cooper, Leah Fitzsimmons, Thomas Jackson, Krishnarajah Nirantharakumar, and Christopher Yau. SurvivEHR: a competing risks, time-to-event foundation model for multiple long-term conditions from primary care electronic health records
-
[15]
Learning the natural history of human disease with generative transformers, June 2024
Artem Shmatko, Alexander Wolfgang Jung, Kumar Gaurav, Søren Brunak, Laust Mortensen, Ewan Birney, Tom Fitzgerald, and Moritz Gerstung. Learning the natural history of human disease with generative transformers, June 2024. URLhttp://medrxiv.org/lookup/doi/1 0.1101/2024.06.07.24308553
2024
-
[16]
DavidePlacido,BoYuan,JessicaX.Hjaltelin,ChunleiZheng,AmalieD.Haue,PiotrJ.Chmura, Chen Yuan, Jihye Kim, Renato Umeton, Gregory Antell, Alexander Chowdhury, Alexandra Franz, Lauren Brais, Elizabeth Andrews, Debora S. Marks, Aviv Regev, Siamack Ayandeh, MaryT.Brophy,NhanV.Do,PeterKraft,BrianM.Wolpin,MichaelH.Rosenthal,NathanaelR. Fillmore,SørenBrunak,andChri...
-
[17]
URLhttps://www.nature.com/articles/s41591-025-04006-w
KaiWang,FeiLiu,WeiWu,ChangxiHu,XianShen,MeihaoWang,GenLi,FanxinZeng,LiLiu, Io Nam Wong, Sian Liu, Zixing Zou, Bingzhou Li, Jinghang Li, Xiaoying Huang, Shengwei Jin, Zhuomin Li, Hui Xu, Gang Chen, Xiaodong Chen, Ying Zhu, Ping Li, Zhe Feng, Winston Wang,LinlingCheng,MingqiYang,QiangHou,WenyangLu,YiwenSun,KunLi,TianZhong, 23 Zhuo Sun, Yun Yin, Alexandre Lo...
-
[18]
Robert Harris, and Rosanna M
Anne Elixhauser, Claudia Steiner, D. Robert Harris, and Rosanna M. Coffey. Comorbidity MeasuresforUsewithAdministrativeData.MedicalCare,36(1),1998. ISSN0025-7079. URL https://journals.lww.com/lww-medicalcare/fulltext/1998/01000/comorbidity _measures_for_use_with_administrative.4.aspx
1998
-
[19]
Mansour T. A. Sharabiani, Paul Aylin, and Alex Bottle. Systematic Review of Comorbidity Indices for Administrative Data.Medical Care, 50(12), 2012. ISSN 0025-7079. URLhttps: //journals.lww.com/lww-medicalcare/fulltext/2012/12000/systematic_review _of_comorbidity_indices_for.14.aspx
2012
-
[20]
Austin, Yu-Ning Wong, Robert G
Steven R. Austin, Yu-Ning Wong, Robert G. Uzzo, J. Robert Beck, and Brian L. Egleston. Why SummaryComorbidityMeasuresSuchAstheCharlsonComorbidityIndexandElixhauserScore Work.MedicalCare, 53(9), 2015. ISSN0025-7079. URLhttps://journals.lww.com/lww -medicalcare/fulltext/2015/09000/why_summary_comorbidity_measures_such_a s_the.14.aspx
2015
-
[21]
Austin, Alison Jennings, Hude Quan, and Alan J
Carl van Walraven, Peter C. Austin, Alison Jennings, Hude Quan, and Alan J. Forster. A Modification of the Elixhauser Comorbidity Measures Into a Point System for Hospital Death Using Administrative Data.Medical Care, 47(6), 2009. ISSN 0025-7079. URLhttps: //journals.lww.com/lww-medicalcare/fulltext/2009/06000/a_modification_of _the_elixhauser_comorbidity.4.aspx
2009
-
[22]
Yanjun Li, Qi Huang, Jin Jiang, Xusheng Du, Wenxin Xiang, Shiqi Zhang, Zean Pan, Liyuan Zhao, Yuyan Cui, Limei Ke, Bo Yin, Linfeng Liu, Guoqing Feng, Shouyi Yan, Liangcai Gao, Yang Liu, Yujuan Yuan, Yanying Guo, Yuqing Yang, Weizhi Ma, Yining Yang, and Qian Di. Large language model-based biological age prediction in large-scale populations.Nature Medicine...
work page doi:10.1038/s4 2025
-
[23]
Amaia Calderón-Larrañaga, Elisa Fabbri, Ana Isabel González, Rafael Perera-Salazar, Nina Grede, BruceGuthrie,JoséMValderas, CaterinaGregorio, ChristianeMuth, DavideLVetrano, GabrieleMeyer,LuigiFerrucci,JeanetWBlom,KerstinBernartz,LaraSchürmann,MariaHanf, Martin Scherer, Michael A Steinman, Mieke Rijken, Sharon Straus, Susan M Smith, Victor M Montori, Svet...
-
[24]
Genevieve Cezard, Calum Thomas McHale, Frank Sullivan, Juliana Kuster Filipe Bowles, and Katherine Keenan. Studying trajectories of multimorbidity: a systematic scoping review of longitudinal approaches and evidence.BMJ Open, 11(11):e048485, November 2021. ISSN 2044-6055, 2044-6055. doi: 10.1136/bmjopen-2020-048485. URLhttps://bmjopen.bmj. com/lookup/doi/...
-
[25]
Michael G Newman, Christina A Porucznik, Ankita P Date, Samir Abdelrahman, Karen C Schliep, James A VanDerslice, Ken R Smith, and Heidi A Hanson. Generating Older Adult Multimorbidity Trajectories Using Various Comorbidity Indices and Calculation Methods.In- novation in Aging, 7(3):igad023, April 2023. ISSN 2399-5300. doi: 10.1093/geroni/igad023. URLhttps...
-
[26]
BERT : Pre-training of Deep Bidirectional Transformers for Language Understanding
Jacob Devlin, Ming-Wei Chang, Kenton Lee, and Kristina Toutanova. BERT: Pre-training of Deep Bidirectional Transformers for Language Understanding. In Jill Burstein, Christy Doran, andThamarSolorio,editors,Proceedingsofthe2019ConferenceoftheNorthAmericanChapter of the Association for Computational Linguistics: Human Language Technologies, Volume 1 (Long a...
-
[27]
NarayanSharma,RenéSchwendimann,OlgaEndrich,DietmarAusserhofer,andMichaelSimon. ComparingCharlsonandElixhausercomorbidityindiceswithdifferentweightingstopredictin- hospital mortality: an analysis of national inpatient data.BMC Health Services Research, 21 (1):13, December 2021. ISSN 1472-6963. doi: 10.1186/s12913-020-05999-5. URLhttps: //bmchealthservres.b...
-
[28]
Beck, Thomas E
Hude Quan, Vijaya Sundararajan, Patricia Halfon, Andrew Fong, Bernard Burnand, Jean- Christophe Luthi, L Duncan Saunders, Cynthia A. Beck, Thomas E. Feasby, and William A. Ghali. CodingAlgorithmsforDefiningComorbiditiesinICD-9-CMandICD-10Administrative Data.Medical Care, 43(11), 2005. ISSN 0025-7079. URLhttps://journals.lww.com/l ww-medicalcare/fulltext/2...
2005
-
[29]
URL https://github.com/ellessenne/comorbidity/
comorbidipy: Python package for calculating comorbidity and clinical risk scores, 2026. URL https://github.com/ellessenne/comorbidity/. 25
2026
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.