EMG-Based Adaptation of Anisotropic Virtual Fixtures for Robot-Assisted Surgical Resection and Dissection
Pith reviewed 2026-06-27 06:42 UTC · model grok-4.3
The pith
EMG signals from forearm muscles let surgeons dynamically expand or disengage anisotropic virtual fixtures during resection and dissection.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
An EMG-driven interface modulates the geometry of an anisotropic virtual fixture so that forearm contractions expand or release the constraint, letting the surgeon switch seamlessly between constrained precise motion and unrestricted repositioning while performing resection and dissection.
What carries the argument
Real-time EMG-based modulation of an anisotropic virtual fixture that expands or disengages on detected forearm muscle intent.
If this is right
- Task accuracy and movement consistency increase relative to fixed-geometry fixtures.
- Perceived cognitive load, physical effort, and frustration decrease for the surgeon.
- The same muscle-signal interface can be applied to other delicate laparoscopic maneuvers.
- Seamless on-the-fly fixture changes reduce the need to switch between different assistance modes manually.
Where Pith is reading between the lines
- The method could be tested in longer procedures to check whether reduced frustration persists over time.
- Combining EMG with other signals such as eye tracking might further improve intent prediction reliability.
- The anisotropic fixture shape might be tuned per procedure type rather than kept generic.
Load-bearing premise
EMG readings from forearm contractions can be mapped reliably to the surgeon's immediate intent without false triggers or noticeable lag.
What would settle it
A controlled trial in which EMG intent detection produces frequent mismatches with actual surgeon goals, resulting in no accuracy gain or added errors during the resection task.
Figures



read the original abstract
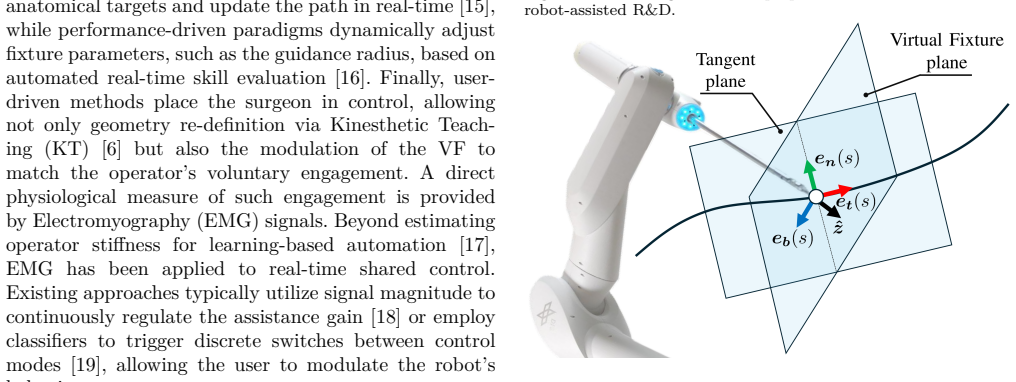
In this paper, we address the development of an adaptive assistance system for robot-assisted laparoscopic surgery, specifically for delicate tasks such as Resection and Dissection. Even if Virtual Fixtures offer significant advantages for guiding a surgeon's movements, conventional Virtual Fixtures are often defined by fixed geometries, lacking the flexibility to adapt to the surgical workflow or the surgeon's immediate intent. To address these limitations, we propose a novel framework for an adaptive and anisotropic virtual fixture. In addition, we introduce an intuitive control interface that modulates the fixture's geometry in real-time based on the surgeon's intent, inferred from EMG signals. This approach allows the surgeon to dynamically expand or disengage the constraint by contracting their forearm muscles, enabling seamless transitions between precise guided motion and free repositioning of the tool. Experimental results from a pilot user study, based on a standardized surgical training task, demonstrate the effectiveness of the proposed method. The system showed significant improvements in task accuracy and movement consistency, alongside a reduction in perceived cognitive load, effort, and frustration.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes a novel framework for adaptive and anisotropic virtual fixtures in robot-assisted laparoscopic surgery for resection and dissection. The fixtures are modulated in real time by an EMG-based interface that infers surgeon intent from forearm muscle contractions, enabling dynamic expansion or disengagement of the constraint. A pilot user study on a standardized surgical training task reports significant gains in task accuracy and movement consistency together with reductions in perceived cognitive load, effort, and frustration.
Significance. If the EMG-based adaptation proves reliable, the work could meaningfully extend virtual-fixture assistance by adding intuitive, intent-driven flexibility without requiring manual mode switches. The combination of anisotropic geometry with real-time EMG modulation addresses a recognized limitation of fixed fixtures and may reduce surgeon workload in delicate tasks; the pilot results, if substantiated with component-level metrics, would constitute a useful empirical demonstration in the human-robot interaction literature for surgical robotics.
major comments (2)
- [Pilot User Study / Results] Pilot User Study / Results: the reported improvements in accuracy, consistency, and NASA-TLX scores are presented only as aggregate task-level outcomes. No EMG-specific metrics (classification accuracy, latency, false-trigger rate, inter-subject variability, or robustness to fatigue/electrode shift) are supplied, so the central attribution of gains to the adaptive mechanism rather than the underlying anisotropic fixture or training effects cannot be verified.
- [Framework Description] Framework Description: the mapping from EMG signal features to fixture modulation commands is described at a high level but lacks quantitative validation of the intent-inference step (e.g., confusion matrix or ROC analysis), which is load-bearing for the claim that the system enables “seamless transitions” based on surgeon intent.
minor comments (2)
- [Abstract] Abstract: the claim of “significant improvements” is stated without any accompanying p-values, effect sizes, or participant count; these details should be added for completeness even in an abstract.
- [Framework] Notation: the precise definition of the anisotropic fixture geometry (e.g., the anisotropy parameters and how they are scaled by the EMG signal) is introduced without an accompanying equation or diagram reference in the early sections.
Simulated Author's Rebuttal
We thank the referee for the constructive comments and the recognition of the work's potential significance. We address each major comment below.
read point-by-point responses
-
Referee: [Pilot User Study / Results] Pilot User Study / Results: the reported improvements in accuracy, consistency, and NASA-TLX scores are presented only as aggregate task-level outcomes. No EMG-specific metrics (classification accuracy, latency, false-trigger rate, inter-subject variability, or robustness to fatigue/electrode shift) are supplied, so the central attribution of gains to the adaptive mechanism rather than the underlying anisotropic fixture or training effects cannot be verified.
Authors: We agree that the pilot study presents only aggregate task-level outcomes without EMG-specific metrics such as classification accuracy, latency, or false-trigger rates. The study was scoped as an initial end-to-end evaluation of the integrated system on a standardized surgical task, with primary outcomes focused on accuracy, consistency, and workload rather than component-level EMG analysis. This does limit the strength of attribution to the adaptive mechanism alone. In revision we will add an explicit limitations subsection acknowledging this gap and outlining future component-level validation. revision_made = partial. revision: partial
-
Referee: [Framework Description] Framework Description: the mapping from EMG signal features to fixture modulation commands is described at a high level but lacks quantitative validation of the intent-inference step (e.g., confusion matrix or ROC analysis), which is load-bearing for the claim that the system enables “seamless transitions” based on surgeon intent.
Authors: The framework description is intentionally concise to emphasize the novel integration of anisotropic fixtures with real-time EMG modulation and the user-study results. We recognize that quantitative validation of the intent-inference step (e.g., confusion matrices) would strengthen claims about seamless transitions. Such detailed classifier metrics were not collected in this pilot. We will revise the framework section to provide additional pipeline details where available and to state the absence of full quantitative validation as a limitation, with plans for future work. revision_made = partial. revision: partial
Circularity Check
No significant circularity; claims rest on empirical user study validation
full rationale
The paper proposes an adaptive anisotropic virtual fixture framework modulated in real time by EMG-inferred surgeon intent and validates effectiveness through a pilot user study on a standardized surgical task, reporting gains in accuracy, consistency, and reduced cognitive load. No mathematical derivation, first-principles prediction, parameter fitting, or uniqueness theorem is presented that could reduce to its own inputs by construction. The central claims are supported by external experimental results rather than self-referential definitions, self-citations, or renamed known patterns, making the work self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
The role of technology in min- imally invasive surgery: state of the art, recent developments and future directions,
M. Tonutti, D. Elson, et al., “The role of technology in min- imally invasive surgery: state of the art, recent developments and future directions,” Postgraduate medical journal, vol. 93, no. 1097, 2017
2017
-
[2]
Robot-assistive minimally invasive surgery: trends and future directions,
G. Dagnino and D. Kundrat, “Robot-assistive minimally invasive surgery: trends and future directions,” International Journal of Intelligent Robotics and Applications, vol. 8, no. 4, 2024
2024
-
[3]
Optimal ergonomics for laparoscopic surgery in minimally invasive surgery suites: a review and guidelines,
M. Van Det, W. Meijerink, et al., “Optimal ergonomics for laparoscopic surgery in minimally invasive surgery suites: a review and guidelines,” Surgical endoscopy, vol. 23, no. 6, 2009
2009
-
[4]
An introduction to roboti- cally assisted surgical systems: current developments and focus areas of research,
J. Klodmann, C. Schlenk, et al., “An introduction to roboti- cally assisted surgical systems: current developments and focus areas of research,” Current Robotics Reports, vol. 2, no. 3, 2021
2021
-
[5]
Gesture recog- nition in robotic surgery: a review,
B. van Amsterdam, M. J. Clarkson, et al., “Gesture recog- nition in robotic surgery: a review,” IEEE Transactions on Biomedical Engineering, vol. 68, no. 6, 2021
2021
-
[6]
Passive virtual fixtures adaptation in minimally invasive robotic surgery,
M. Selvaggio, G. A. Fontanelli, et al., “Passive virtual fixtures adaptation in minimally invasive robotic surgery,” IEEE Robotics and Automation Letters, vol. 3, no. 4, 2018
2018
-
[7]
Active constraints/virtual fixtures: A survey,
S. A. Bowyer, B. L. Davies, et al., “Active constraints/virtual fixtures: A survey,” IEEE Transactions on Robotics, vol. 30, no. 1, 2013
2013
-
[8]
Haptic virtual fixtures for robot-assisted manipulation,
J. J. Abbott, P. Marayong, et al., “Haptic virtual fixtures for robot-assisted manipulation,” in Robotics Research. Springer, 2007
2007
-
[9]
Active compliance in robotic surgery—the use of force control as a dynamic constraint,
B. Davies, S. Harris, et al., “Active compliance in robotic surgery—the use of force control as a dynamic constraint,” Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, vol. 211, no. 4, 1997
1997
-
[10]
Anatomical mesh-based virtual fixtures for surgical robots,
Z. Li, A. Gordon, et al., “Anatomical mesh-based virtual fixtures for surgical robots,” in 2020 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS). IEEE, 2020
2020
-
[11]
Virtual fixtures assistance for safe polyp dissection in minimally invasive robotic surgery,
J. Feng, X. Li, et al., “Virtual fixtures assistance for safe polyp dissection in minimally invasive robotic surgery,” in 2021 5th International Conference on Automation, Control and Robots (ICACR). IEEE, 2021
2021
-
[12]
Active constraints using vector field inequalities for surgical robots,
M. M. Marinho, B. V. Adorno, et al., “Active constraints using vector field inequalities for surgical robots,” in 2018 IEEE International Conference on Robotics and Automation (ICRA). IEEE, 2018
2018
-
[13]
A virtual fixtures control method of surgical robot based on human arm kinematics model,
A. Lin, Y. Tang, et al., “A virtual fixtures control method of surgical robot based on human arm kinematics model,” IEEE Access, vol. 7, 2019
2019
-
[14]
Vision-based dynamic virtual fixtures for tools collision avoidance in robotic surgery,
R. Moccia, C. Iacono, et al., “Vision-based dynamic virtual fixtures for tools collision avoidance in robotic surgery,” IEEE Robotics and Automation Letters, vol. 5, no. 2, 2020
2020
-
[15]
Vision-based virtual fixtures generation for robotic-assisted polyp dissection procedures,
R. Moccia, M. Selvaggio, et al., “Vision-based virtual fixtures generation for robotic-assisted polyp dissection procedures,” in 2019 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS). IEEE, 2019
2019
-
[16]
A dual-user teleoperated system with virtual fixtures for robotic surgical training,
M. Shahbazi, S. F. Atashzar, et al., “A dual-user teleoperated system with virtual fixtures for robotic surgical training,” in 2013 IEEE International Conference on Robotics and Automation. IEEE, 2013
2013
-
[17]
Learning from demonstration of robot motions and stiffness behaviors for surgical blunt dissection,
R. Arduini, Y. Michel, et al., “Learning from demonstration of robot motions and stiffness behaviors for surgical blunt dissection,” in 2024 33rd IEEE International Conference on Robot and Human Interactive Communication (ROMAN). IEEE, 2024
2024
-
[18]
A regulable linear guidance flexible virtual fixture based on EMG in teleoperation system,
Y. Fan, J. Luo, et al., “A regulable linear guidance flexible virtual fixture based on EMG in teleoperation system,” in 2021 26th International Conference on Automation and Computing (ICAC). IEEE, 2021
2021
-
[19]
EMG-driven shared control architecture for human–robot co-manipulation tasks,
F. Patriarca, P. Di Lillo, et al., “EMG-driven shared control architecture for human–robot co-manipulation tasks,” Ma- chines, vol. 13, no. 8, 2025
2025
-
[20]
Optimizing design and control methods for using collaborative robots in upper limb rehabilitation,
D. Onfiani, M. Caramaschi, et al., “Optimizing design and control methods for using collaborative robots in upper limb rehabilitation,” IEEE/ASME Transactions on Mechatronics, 2025
2025
-
[21]
Vision assisted control for manipulation using virtual fixtures,
A. Bettini, P. Marayong, et al., “Vision assisted control for manipulation using virtual fixtures,” IEEE Transactions on Robotics, vol. 20, no. 6, 2004
2004
-
[22]
Evaluating and exploring the myo armband,
S. Rawat, S. Vats, et al., “Evaluating and exploring the myo armband,” in 2016 International Conference System Modeling & Advancement in Research Trends (SMART). IEEE, 2016
2016
-
[23]
The DLR mirosurge surgical robotic demonstrator,
U. Seibold, B. Kübler, T. Bahls, R. Haslinger, and F. Steidle, “The DLR mirosurge surgical robotic demonstrator,” in The Encyclopedia of MEDICAL ROBOTICS: Volume 1 Minimally Invasive Surgical Robotics. World Scientific, 2019
2019
-
[24]
Further development of a backdrivable linear axis for collaborative laparoscopic surgery,
S. Müller-Spahn, “Further development of a backdrivable linear axis for collaborative laparoscopic surgery,” Master’s thesis, Institut für Robotik und Mechatronik, 2024. [Online]. A vailable:https://elib.dlr.de/204413/
2024
-
[25]
Mimo state feedback controller for a flexible joint robot with strong joint coupling,
L. Le Tien, A. A. Schaffer, and G. Hirzinger, “Mimo state feedback controller for a flexible joint robot with strong joint coupling,” in Proceedings 2007 IEEE International Conference on Robotics and Automation. IEEE, 2007
2007
-
[26]
Friction observer and compensation for control of robots with joint torque measurement,
L. Le Tien, A. Albu-Schaffer, A. De Luca, and G. Hirzinger, “Friction observer and compensation for control of robots with joint torque measurement,” in 2008 IEEE/RSJ International Conference on Intelligent Robots and Systems. IEEE, 2008
2008
-
[27]
Hierarchical impedance-based track- ing control of kinematically redundant robots,
A. Dietrich and C. Ott, “Hierarchical impedance-based track- ing control of kinematically redundant robots,” IEEE Trans- actions on Robotics, vol. 36, no. 1, 2019
2019
-
[28]
Cartesian impedance control of redundant robots: recent results with the dlr-light-weight-arms,
A. Albu-Schaffer, C. Ott, U. Frese, and G. Hirzinger, “Cartesian impedance control of redundant robots: recent results with the dlr-light-weight-arms,” in 2003 IEEE In- ternational Conference on Robotics and Automation (Cat. No.03CH37422), vol. 3, 2003
2003
-
[29]
Lübecker toolbox training exer- cises,
Lübeck Toolbox Ltd., “Lübecker toolbox training exer- cises,” http://www.luebeck-toolbox.com/training.html, ac- cessed: 2024-01-24
2024
-
[30]
Thomaschewski, T
M. Thomaschewski, T. Laubert, et al., “Efficacy of goal- directed minimally invasive surgery simulation training with the lübeck toolbox-curriculum prior to first operations on pa- tients: Study protocol for a multi-centre randomized controlled validation trial (novice),” International Journal of Surgery Protocols, vol. 21, 2020
2020
-
[31]
Thomaschewski, M
M. Thomaschewski, M. Kist, et al., “Conception and prospec- tive multicentric validation of a robotic surgery training curriculum (rostrac) for surgical residents: from simulation via laboratory training to integration into the operation room,” Journal of Robotic Surgery, vol. 18, no. 1, 2024
2024
-
[32]
R. Budiu. (2018) Between-subjects vs. within-subjects study design. Nielsen Norman Group. Accessed: 2025-02-
2018
-
[33]
A vailable: https://www.nngroup.com/articles/ between-within-subjects/
[Online]. A vailable: https://www.nngroup.com/articles/ between-within-subjects/
-
[34]
Development of NASA- TLX (task load index): Results of empirical and theoretical research,
S. G. Hart and L. E. Staveland, “Development of NASA- TLX (task load index): Results of empirical and theoretical research,” Advances in Psychology, vol. 52, 1988
1988
-
[35]
SUS: A quick and dirty usability scale,
J. Brooke, “SUS: A quick and dirty usability scale,” Digital Equipment Co., Reading, UK, Tech. Rep. TR-26, 1996
1996
-
[36]
Mixed-effects modeling with crossed random effects for subjects and items,
R. H. Baayen, D. J. Davidson, et al., “Mixed-effects modeling with crossed random effects for subjects and items,” Journal of memory and language, vol. 59, no. 4, 2008
2008
-
[37]
Collision detection and reaction: A contribution to safe physical human-robot interaction,
S. Haddadin, A. Albu-Schaffer, et al., “Collision detection and reaction: A contribution to safe physical human-robot interaction,” in 2008 IEEE/RSJ International Conference on Intelligent Robots and Systems. IEEE, 2008
2008
-
[38]
An empirical evaluation of the system usability scale,
A. Bangor, P. T. Kortum, et al., “An empirical evaluation of the system usability scale,” International Journal of Human- Computer Interaction, vol. 24, no. 6, 2008
2008
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.