Patient-Level Elbow Abnormality Detection: Leakage-Aware Evaluation of Learned Preprocessing, Calibration, and Triage-Oriented Operating Points
Pith reviewed 2026-07-01 05:53 UTC · model grok-4.3
The pith
No preprocessing strategy shows consistent advantage over raw DenseNet121 in patient-level elbow abnormality detection.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
In a leakage-aware evaluation on elbow radiographs, preprocessing pipelines with and without a DnCNN module were compared to a raw-input DenseNet121 baseline for patient-level abnormality detection. Differences in performance were modest and configuration-dependent, with no strategy achieving consistent gains in AUROC, PR-AUC, ECE, or Brier score. The raw-input baseline stayed competitive, and certain raw plus DnCNN combinations even lowered calibration errors while CLAHE with DnCNN did not.
What carries the argument
Leakage-aware patient-level protocol that keeps all images from one patient in a single data split to prevent leakage.
If this is right
- Preprocessing effects depend on the specific combination of methods and metrics used.
- Raw inputs with DnCNN front-end can reduce expected calibration error and Brier score.
- CLAHE preprocessing combined with DnCNN fails to improve calibration.
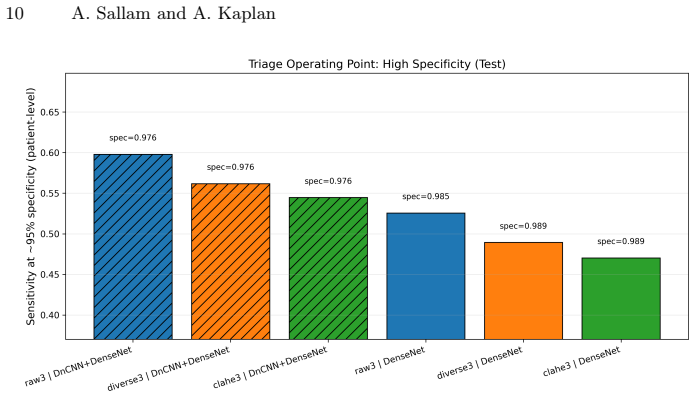
- Validation-selected operating points allow targeting high specificity for triage.
Where Pith is reading between the lines
- Similar modest preprocessing effects may appear in other radiograph-based detection tasks if patient-level splits are enforced.
- Efforts to develop new preprocessing might be better directed toward improving model architectures or data collection instead.
- Repeating the experiments on different anatomical regions could test the generality of the baseline's competitiveness.
Load-bearing premise
That the patient-level split fully eliminates leakage while preserving enough data for reliable training and testing.
What would settle it
A preprocessing pipeline that outperforms the raw DenseNet121 baseline on all metrics (AUROC, PR-AUC, ECE, Brier) consistently across repeated patient-level splits would falsify the claim of no consistent advantage.
Figures
read the original abstract
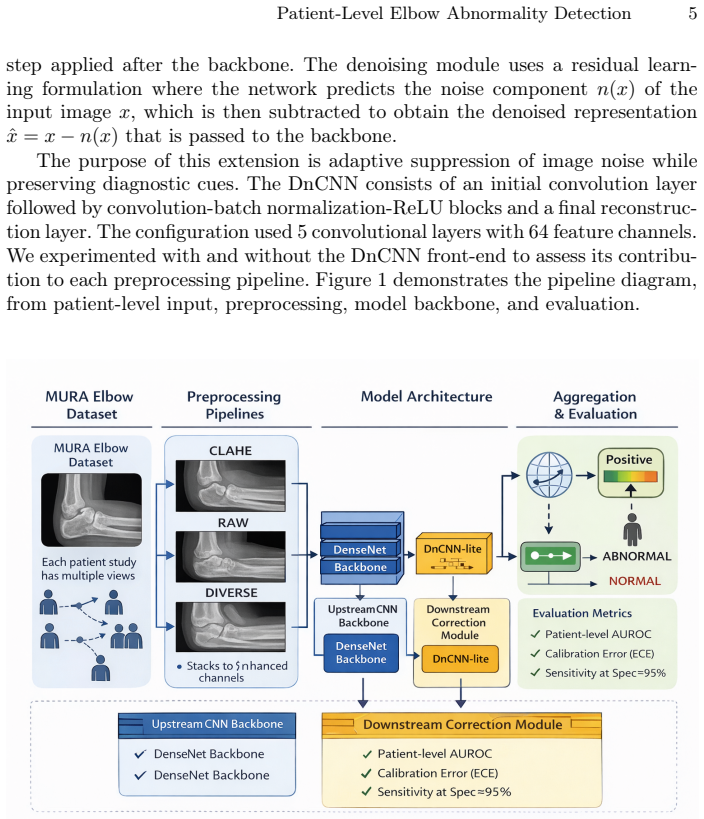
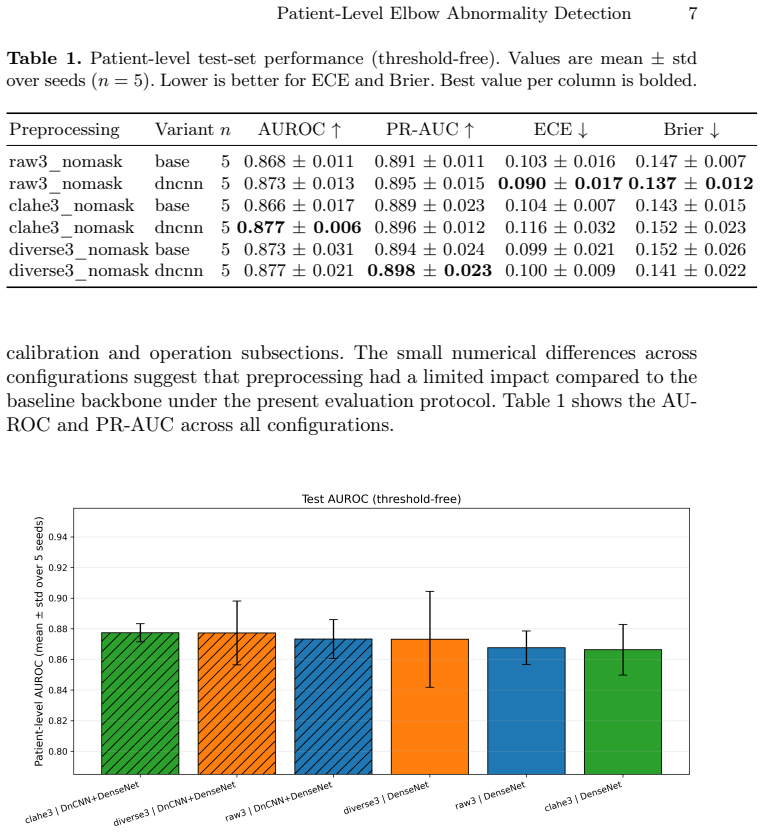
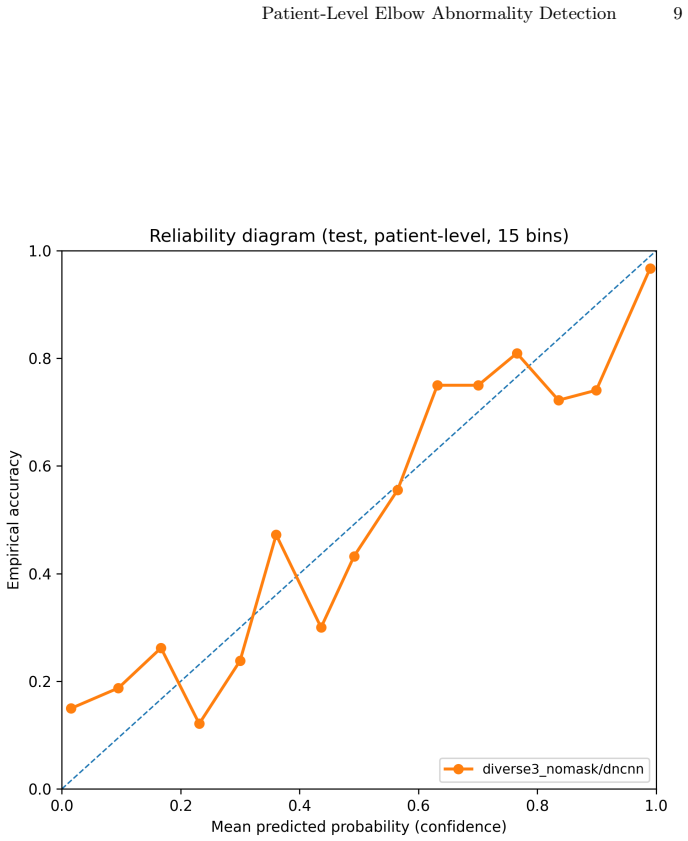
In this study, we examine learned preprocessing pipelines in the context of triage-oriented orthopedic abnormality detection task using elbow radiographs from MURA dataset. The evaluation focuses on patient-level detection of musculoskeletal abnormalities under a leakage-aware protocol. We compare multiple preprocessing pipelines, with and without a lightweight DnCNN module as a learned preprocessing component, to assess their impact on discrimination and calibration. Performance is assessed using discrimination metrics (AUROC, PR-AUC), calibration measures (ECE, Brier score), and validation-selected operating point analysis targeting high specificity. Results show that differences across preprocessing strategies are modest and configuration-dependent, with no consistent discrimination advantage over the raw-input DenseNet121 baseline. The raw and diverse inputs combined with the DnCNN front-end showed reduced ECE and Brier score, while CLAHE combined with DnCNN did not improve calibration. Overall, the results suggest that under patient-level evaluation, preprocessing gains are modest and configuration-dependent; the raw-input DenseNet121 baseline remains competitive throughout, and no tested preprocessing strategy produced a consistent discrimination advantage across all metrics.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript reports an empirical comparison of preprocessing pipelines (including DnCNN-based learned preprocessing) versus a raw-input DenseNet121 baseline for patient-level elbow abnormality detection on the MURA dataset. Under a leakage-aware patient-level split, it finds that differences in AUROC and PR-AUC are modest and configuration-dependent, with no preprocessing strategy showing consistent discrimination gains; some raw+DnCNN and diverse-input combinations improve calibration (ECE, Brier), while CLAHE+DnCNN does not. The raw baseline remains competitive across metrics and high-specificity operating points.
Significance. If the leakage-aware protocol and modest differences hold under scrutiny, the result is useful for triage-oriented deployment: it indicates that added preprocessing complexity does not reliably improve discrimination on this task and dataset, supporting simpler baselines. The multi-metric evaluation (discrimination + calibration + operating-point analysis) and explicit patient-level focus are strengths that align with clinical requirements.
major comments (2)
- [§3] §3 (Methods, leakage-aware protocol): The patient-level split is described as preventing same-patient images across train/val/test, but exact grouping rules, patient counts per split, and verification that no intra-patient leakage occurred are not quantified; this is load-bearing for the central claim that all comparisons are leakage-free and that the baseline remains competitive.
- [§4] §4 (Results, discrimination tables): The claim of 'no consistent discrimination advantage' rests on modest AUROC/PR-AUC differences, yet no statistical tests (e.g., DeLong or bootstrap CIs) or effect-size measures are reported for pairwise comparisons against the raw baseline; without these, it is unclear whether observed differences are robust or merely sampling variation.
minor comments (2)
- [Table 2] Table 2 and Figure 3: axis labels and legend entries for the DnCNN variants are abbreviated without a clear key, making it difficult to map configurations to the text descriptions.
- [§5] §5 (Discussion): The statement that 'preprocessing gains are modest' would benefit from a short quantitative summary (e.g., maximum observed AUROC delta) rather than qualitative description only.
Simulated Author's Rebuttal
We thank the referee for the constructive review and the recommendation for minor revision. The comments correctly identify areas where additional detail and statistical support would strengthen the presentation of the leakage-aware protocol and the discrimination results. We respond to each major comment below.
read point-by-point responses
-
Referee: [§3] §3 (Methods, leakage-aware protocol): The patient-level split is described as preventing same-patient images across train/val/test, but exact grouping rules, patient counts per split, and verification that no intra-patient leakage occurred are not quantified; this is load-bearing for the central claim that all comparisons are leakage-free and that the baseline remains competitive.
Authors: We agree that the description would benefit from explicit quantification. The current manuscript states that the split is performed at the patient level using unique patient identifiers, but does not report the resulting patient counts or the precise verification steps. In the revision we will add the number of patients (and images) in each split together with a concise statement of the grouping procedure and the check performed to confirm no patient ID appears in more than one partition. revision: yes
-
Referee: [§4] §4 (Results, discrimination tables): The claim of 'no consistent discrimination advantage' rests on modest AUROC/PR-AUC differences, yet no statistical tests (e.g., DeLong or bootstrap CIs) or effect-size measures are reported for pairwise comparisons against the raw baseline; without these, it is unclear whether observed differences are robust or merely sampling variation.
Authors: We accept the point. While the observed AUROC and PR-AUC differences are small and the raw baseline remains competitive across all tested configurations and secondary metrics, the absence of formal statistical comparison leaves the robustness of those differences unquantified. In the revised manuscript we will report bootstrap confidence intervals for the AUROC differences (or DeLong tests where appropriate) between each preprocessing variant and the raw DenseNet121 baseline. revision: yes
Circularity Check
Empirical evaluation with no derivation chain or self-referential claims
full rationale
The paper is a purely empirical comparison of preprocessing pipelines (including DnCNN variants) on the MURA elbow radiographs under a patient-level leakage-aware split. No equations, mathematical derivations, uniqueness theorems, or parameter fits are presented that could reduce to their own inputs. The central claim—that no tested strategy yields a consistent discrimination advantage over the raw DenseNet121 baseline—is a direct reporting of observed AUROC, PR-AUC, ECE, and Brier scores across configurations. This is self-contained against external benchmarks and contains no load-bearing self-citations or ansatzes. Honest non-finding applies.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption The MURA dataset provides reliable labels for elbow abnormalities and the patient-level splits can be made without leakage.
Reference graph
Works this paper leans on
-
[1]
Acta Biomedica89(1-S), 111–123 (2018)
Pinto, A., Berritto, D., Russo, A., Riccitiello, F., Caruso, M., Belfiore, M.P., Papapietro, V.R., Carotti, M., Pinto, F., Giovagnoni, A., Romano, L., Grassi, R.: Traumatic fractures in adults: missed diagnosis on plain radio- graphs in the Emergency Department. Acta Biomedica89(1-S), 111–123 (2018). https://doi.org/10.23750/abm.v89i1-S.7015
-
[2]
Journal of Emergency Nursing39(4), 398–408 (2013)
Robinson, D.J.: An Integrative Review: Triage Protocols and the Effect on ED Length of Stay. Journal of Emergency Nursing39(4), 398–408 (2013). https://doi.org/10.1016/j.jen.2011.12.016 12 A. Sallam and A. Kaplan
-
[3]
BMC Musculoskeletal Disorders21(1), 510 (2020)
Samsson, K.S., Larsson, M.E.H.: Effects on health and process outcomes of physiotherapist-led orthopaedic triage for patients with musculoskeletal disorders: a systematic review of comparative studies. BMC Musculoskeletal Disorders21(1), 510 (2020). https://doi.org/10.1186/s12891-020-03673-9
-
[4]
MURA: Large Dataset for Abnormality Detection in Musculoskeletal Radiographs
Rajpurkar, P., Irvin, J., Bagul, A., Ding, D., Duan, T., Mehta, H., Yang, B., Zhu, K., Laird, D., Ball, R.L., Langlotz, C., Shpanskaya, K., Lungren, M.P., Ng, A.Y.: MURA: Large Dataset for Abnormality Detection in Musculoskeletal Radiographs. arXiv preprint arXiv:1712.06957 (2018)
work page internal anchor Pith review Pith/arXiv arXiv 2018
-
[5]
Applied Sciences10(4), 1507 (2020)
Tanzi, L., Vezzetti, E., Moreno, R., Moos, S.: X-Ray Bone Fracture Classifica- tion Using Deep Learning: A Baseline for Designing a Reliable Approach. Applied Sciences10(4), 1507 (2020). https://doi.org/10.3390/app10041507
-
[6]
Clinical Radiology79(11), e1394–e1402 (2024)
Tahir, A., Saadia, A., Khan, K., Gul, A., Qahmash, A., Akram, R.N.: Enhancing diagnosis: ensemble deep-learning model for fracture detec- tion using X-ray images. Clinical Radiology79(11), e1394–e1402 (2024). https://doi.org/10.1016/j.crad.2024.08.006
-
[7]
Diagnostics12(10), 2420 (2022)
Meena, T., Roy, S.: Bone Fracture Detection Using Deep Supervised Learning from Radiological Images: A Paradigm Shift. Diagnostics12(10), 2420 (2022). https://doi.org/10.3390/diagnostics12102420
-
[8]
Scientific Reports14(1), 23053 (2024)
Husarek, J., Hess, S., Razaeian, S., et al.: Artificial intelligence in commercial frac- ture detection products: a systematic review and meta-analysis of diagnostic test accuracy. Scientific Reports14(1), 23053 (2024). https://doi.org/10.1038/s41598- 024-73058-8
-
[9]
Materials Today: Proceedings80, 2557– 2562 (2023)
Karanam, S.R., Srinivas, Y., Chakravarty, S.: A systematic review on approach and analysis of bone fracture classification. Materials Today: Proceedings80, 2557– 2562 (2023). https://doi.org/10.1016/j.matpr.2021.06.408
-
[10]
Kuo, R.Y.L., Harrison, C., Curran, T.A., Jones, B., Freethy, A., Cussons, D., Stewart, M., Collins, G.S., Furniss, D.: Artificial Intelligence in Fracture Detec- tion: A Systematic Review and Meta-Analysis. Radiology304(1), 50–62 (2022). https://doi.org/10.1148/radiol.211785
-
[11]
PLOS Digital Health3(1), e0000438 (2024)
Jung, J., Dai, J., Liu, B., Wu, Q.: Artificial intelligence in fracture de- tection with different image modalities and data types: A systematic review and meta-analysis. PLOS Digital Health3(1), e0000438 (2024). https://doi.org/10.1371/journal.pdig.0000438
-
[12]
NPJ Digital Medicine 3, 144 (2020)
Jones, R.M., Sharma, A., Hotchkiss, R., et al.: Assessment of a deep-learning sys- tem for fracture detection in musculoskeletal radiographs. NPJ Digital Medicine 3, 144 (2020). https://doi.org/10.1038/s41746-020-00352-w
-
[13]
In: Drukker, K., Mazurowski, M.A
Luo, J., Kitamura, G., Doganay, E., Arefan, D., Wu, S.: Medical knowledge- guided deep curriculum learning for elbow fracture diagnosis from X-ray images. In: Drukker, K., Mazurowski, M.A. (eds.) Medical Imaging 2021: Computer-Aided Diagnosis. SPIE (2021). https://doi.org/10.1117/12.2582184
-
[14]
Quantitative Imaging in Medicine and Surgery15(3), 2529–2546 (2025)
Wu, Y., Fong, S., Yu, J.: Enhancing bone radiology images classification through appropriate preprocessing: a deep learning and explainable artificial intelligence approach. Quantitative Imaging in Medicine and Surgery15(3), 2529–2546 (2025). https://doi.org/10.21037/qims-24-1745
-
[15]
IEEE Transactions on Image Processing26(7), 3142–3155 (2017)
Zhang, K., Zuo, W., Chen, Y., Meng, D., Zhang, L.: Beyond a Gaussian Denoiser: Residual Learning of Deep CNN for Image Denoising. IEEE Transactions on Image Processing26(7), 3142–3155 (2017). https://doi.org/10.1109/tip.2017.2662206
-
[16]
Sharan, T.S., Bhattacharjee, R., Sharma, S., Sharma, N.: Evaluation of Deep Learning Methods (DnCNN and U-Net) for Denoising of Heart Ausculta- tion Signals. In: 2020 3rd International Conference on Communication Sys- Patient-Level Elbow Abnormality Detection 13 tem, Computing and IT Applications (CSCITA), pp. 151–155. IEEE (2020). https://doi.org/10.1109...
-
[17]
Kangralkar, V., Hulmani, V., Nasery, T., Shilaskar, S.: Image Denoising with DnCNN and Autoencoder: A Deep Learning Approach. In: Nanda, S.J., et al. (eds.) Data Science and Applications, pp. 323–336. Springer, Singapore (2025). https://doi.org/10.1007/978-981-96-2299-3_22
-
[18]
MONAI: An open-source framework for deep learning in healthcare
Cardoso, M.J., et al.: MONAI: An open-source framework for deep learning in healthcare. arXiv preprint arXiv:2211.02701 (2022)
work page internal anchor Pith review Pith/arXiv arXiv 2022
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.