Few-Shot Left Atrial Wall Segmentation in 3D LGE MRI via Meta-Learning
Pith reviewed 2026-05-15 00:49 UTC · model grok-4.3
The pith
Meta-learning with auxiliary cavity tasks improves few-shot accuracy for thin left atrial wall segmentation in 3D MRI.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The MAML framework meta-trained on the wall task together with auxiliary left and right atrial cavity tasks and uses a boundary-aware composite loss to emphasize thin-structure accuracy. On the hold-out test set it improves segmentation over supervised fine-tuning, reaching a Dice score of 0.64 versus 0.52 and an HD95 of 5.70 mm versus 7.60 mm at five shots, and approaches the fully supervised reference of 0.71 Dice at twenty shots. The gains persist, though reduced, under synthetic shift and on the local cohort.
What carries the argument
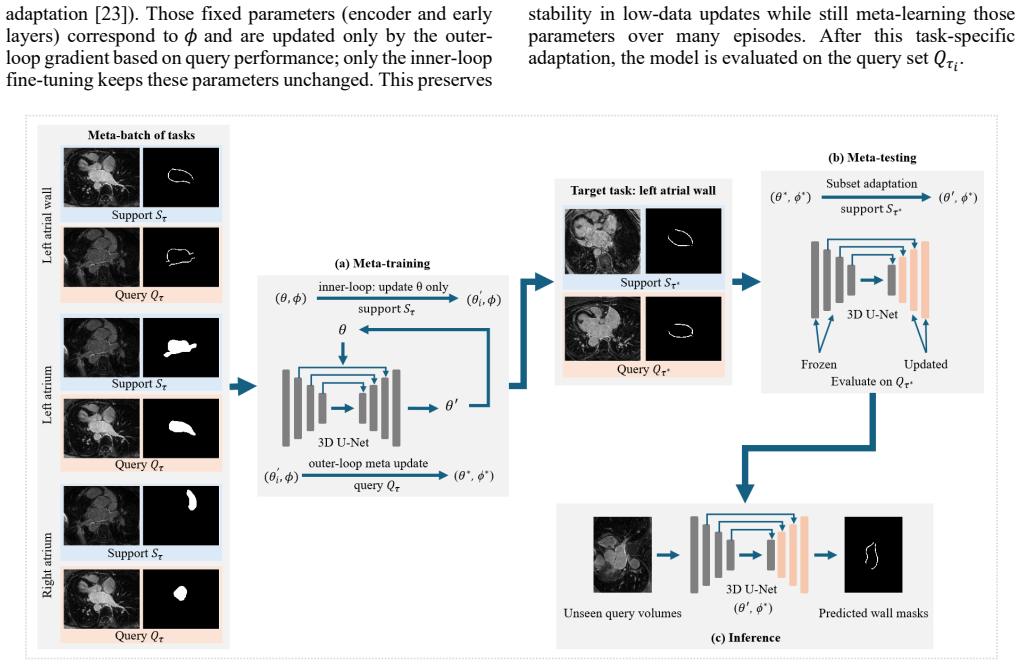
Model-Agnostic Meta-Learning (MAML) meta-trained jointly on the thin-wall segmentation task plus auxiliary left and right atrial cavity tasks, guided by a boundary-aware composite loss.
If this is right
- At five shots the meta-trained model reaches 0.64 Dice and 5.70 mm HD95 on hold-out data versus 0.52 Dice and 7.60 mm for fine-tuning.
- Under an unseen synthetic domain shift the same five-shot model still attains 0.59 Dice and 5.99 mm HD95.
- Performance on a distinct local cohort remains competitive at 0.57 Dice for five shots and rises with more shots.
- At twenty shots the meta-trained model reaches 0.69 Dice, nearly matching the fully supervised reference of 0.71.
Where Pith is reading between the lines
- The same joint meta-training pattern could be tested on other thin-walled structures such as vessel walls or cortical layers where annotations are costly.
- If the auxiliary-task benefit holds, the labeling burden for new clinical sites could drop from hundreds of volumes to a handful, speeding routine use of 3D atrial remodeling assessment.
- The boundary-aware loss term may be worth isolating in future ablations to check whether it alone explains most of the thin-structure gains.
Load-bearing premise
The auxiliary cavity segmentation tasks share enough structure with the thin-wall task that meta-training transfers useful knowledge to new data.
What would settle it
Running the identical MAML setup without the auxiliary cavity tasks on the five-shot hold-out test set and finding no Dice or HD95 improvement over standard fine-tuning would falsify the central claim.
Figures

read the original abstract
Segmenting the left atrial wall from late gadolinium enhancement magnetic resonance images (MRI) is challenging due to the wall's thin geometry, low contrast, and the scarcity of expert annotations. We propose a Model-Agnostic Meta-Learning (MAML) framework for K-shot (K = 5, 10, 20) 3D left atrial wall segmentation that is meta-trained on the wall task together with auxiliary left atrial and right atrial cavity tasks and uses a boundary-aware composite loss to emphasize thin-structure accuracy. We evaluated MAML segmentation performance on a hold-out test set and assessed robustness under an unseen synthetic shift and on a distinct local cohort. On the hold-out test set, MAML appeared to improve segmentation performance compared to the supervised fine-tuning model, achieving a Dice score (DSC) of 0.64 vs. 0.52 and HD95 of 5.70 vs. 7.60 mm at 5-shot, and approached the fully supervised reference at 20-shot (0.69 vs. 0.71 DSC). Under unseen shift, performance degraded but remained robust: at 5-shot, MAML attained 0.59 DSC and 5.99 mm HD95 on the unseen domain shift and 0.57 DSC and 6.01 mm HD95 on the local cohort, with consistent gains as K increased. These results suggest that more accurate and reliable thin-wall boundaries are achievable in low-shot adaptation, potentially enabling clinical translation with minimal additional labeling for the assessment of atrial remodeling.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper claims that a MAML framework meta-trained jointly on the left atrial wall segmentation task plus auxiliary left and right atrial cavity tasks, combined with a boundary-aware composite loss, enables effective K-shot (K=5,10,20) 3D wall segmentation in LGE MRI. It reports improved performance over supervised fine-tuning baselines (DSC 0.64 vs. 0.52 and HD95 5.70 vs. 7.60 mm at 5-shot on hold-out data) that approaches fully supervised results at 20-shot, with maintained robustness under synthetic domain shift and on a local cohort.
Significance. If the meta-transfer from auxiliary cavity tasks to thin-wall segmentation is confirmed, the work would be significant for few-shot medical image segmentation by reducing annotation burden for thin, low-contrast structures relevant to atrial remodeling assessment. The multi-cohort evaluation (hold-out, synthetic shift, local) is a strength that supports robustness claims. Credit is given for the explicit K-shot protocol and boundary-aware loss design.
major comments (2)
- [Methods] Methods section: the central claim that auxiliary cavity tasks provide useful inductive bias for meta-transfer to the thin-wall task is load-bearing, yet no ablation is described that trains MAML on the wall task alone (without cavities) or compares against a non-meta model using only the boundary-aware loss; without this, the DSC gain (0.64 vs. 0.52) cannot be attributed to MAML rather than the loss.
- [Results] Results section: reported quantitative improvements (DSC, HD95) lack statistical tests, standard deviations across runs, or confidence intervals, so it is unclear whether the observed gains over supervised fine-tuning are statistically reliable given the small K-shot regimes and test-set sizes.
minor comments (1)
- [Abstract] Abstract: the statement that performance 'approached the fully supervised reference at 20-shot (0.69 vs. 0.71 DSC)' would benefit from explicitly stating the fully supervised DSC value and whether the difference is within expected variance.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback, which highlights important aspects of our experimental design and reporting. We address each major comment below and will update the manuscript to strengthen the claims regarding the contribution of auxiliary tasks and to include appropriate statistical analysis.
read point-by-point responses
-
Referee: [Methods] Methods section: the central claim that auxiliary cavity tasks provide useful inductive bias for meta-transfer to the thin-wall task is load-bearing, yet no ablation is described that trains MAML on the wall task alone (without cavities) or compares against a non-meta model using only the boundary-aware loss; without this, the DSC gain (0.64 vs. 0.52) cannot be attributed to MAML rather than the loss.
Authors: We agree that the current manuscript lacks the necessary ablations to isolate the effect of the auxiliary cavity tasks within the MAML framework and to separate the contribution of meta-learning from the boundary-aware loss. In the revised version, we will add an ablation study that includes: (1) MAML trained solely on the wall segmentation task without auxiliary cavities, and (2) a non-meta supervised baseline using only the boundary-aware composite loss. These results will be reported alongside the main experiments to clarify the source of the observed performance gains. revision: yes
-
Referee: [Results] Results section: reported quantitative improvements (DSC, HD95) lack statistical tests, standard deviations across runs, or confidence intervals, so it is unclear whether the observed gains over supervised fine-tuning are statistically reliable given the small K-shot regimes and test-set sizes.
Authors: We acknowledge that the reported metrics would benefit from statistical rigor to confirm reliability, especially in low-shot settings. In the revision, we will rerun the experiments across multiple random seeds for K-shot task sampling, report mean and standard deviation for DSC and HD95, and include paired statistical tests (e.g., Wilcoxon signed-rank test) with p-values to assess significance of differences versus the fine-tuning baseline. Confidence intervals will also be added where feasible. revision: yes
Circularity Check
No significant circularity; empirical results measured on independent test sets
full rationale
The paper reports an empirical MAML-based segmentation method evaluated via direct measurement of DSC and HD95 on hold-out test sets, an unseen synthetic shift, and a distinct local cohort. Performance numbers are obtained from model inference on separate data rather than derived from any fitted parameter or self-referential equation. No self-definitional loops, fitted-input predictions, or load-bearing self-citations appear in the derivation; the auxiliary-task meta-training and boundary-aware loss are standard components whose benefit is assessed by ablation-free but externally measured comparison to supervised fine-tuning. The chain remains self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
free parameters (1)
- K (number of shots)
axioms (1)
- domain assumption Auxiliary left and right atrial cavity segmentation tasks share sufficient structure with the thin-wall task to support positive meta-transfer.
Reference graph
Works this paper leans on
-
[1]
Y. Wu, Z. Tang, B. Li, D. Firmin, and G. Yang, “Recent Advances in Fibrosis and Scar Segmentation From Cardiac MRI: A State-of-the-Art Review and Future Perspectives,” Front. Physiol., vol. 12, p. 709230, Aug. 2021, doi: 10.3389/FPHYS.2021.709230
-
[2]
RAS Dataset: A 3D Cardiac LGE -MRI Dataset for Segmentation of Right Atrial Cavity,
J. Zhu et al. , “RAS Dataset: A 3D Cardiac LGE -MRI Dataset for Segmentation of Right Atrial Cavity,” Sci. Data, vol. 11, no. 1, p. 401, Dec. 2024, doi: 10.1038/S41597-024-03253-9
-
[3]
The use of MRI in quantification of the atrial fibrosis in patients with rheumatic mitral disease,
A. S. Ismail, Y. Baghdady, M. A. Salem, and A. A. Wahab, “The use of MRI in quantification of the atrial fibrosis in patients with rheumatic mitral disease,” Egyptian Journal of Radiology and Nuclear Medicine, vol. 51, no. 1, Dec. 2020, doi: 10.1186/s43055-020-00322-y
-
[4]
Left atrial fibrosis in atrial fibrillation: Mechanisms, clinical evaluation and management,
J. Ma, Q. Chen, and S. Ma, “Left atrial fibrosis in atrial fibrillation: Mechanisms, clinical evaluation and management,” Mar. 01, 2021, John Wiley and Sons Inc. doi: 10.1111/jcmm.16350
-
[5]
Medical image analysis on left atrial LGE MRI for atrial fibrillation studies: A review,
L. Li, V. A. Zimmer, J. A. Schnabel, and X. Zhuang, “Medical Image Analysis on Left Atrial LGE MRI for Atrial Fibrillation Studies: A Review,” Med. Image Anal. , vol. 77, p. 102360, Apr. 2022, doi: 10.1016/J.MEDIA.2022.102360
-
[6]
Usformer: A small network for left atrium segmentation of 3D LGE MRI,
H. Lin et al., “Usformer: A small network for left atrium segmentation of 3D LGE MRI,” Heliyon, vol. 10, no. 7, Apr. 2024, doi: 10.1016/j.heliyon.2024.e28539
-
[7]
Z. Xiong et al., “A global benchmark of algorithms for segmenting the left atrium from late gadolinium-enhanced cardiac magnetic resonance imaging,” Med. Image Anal. , vol. 67, Jan. 2021, doi: 10.1016/j.media.2020.101832
-
[8]
G. Yang et al. , “Simultaneous left atrium anatomy and scar segmentations via deep learning in multiview information with attention,” Future Generation Computer Systems , vol. 107, pp. 215 – 228, Jun. 2020, doi: 10.1016/j.future.2020.02.005
-
[9]
L. Li, V. A. Zimmer, J. A. Schnabel, and X. Zhuang, “AtrialJSQnet: A New framework for joint segmentation and quantification of left atrium and scars incorporating spatial and shape information,” Med. Image Anal., vol. 76, Feb. 2022, doi: 10.1016/j.media.2021.102303
-
[10]
C. Thesing, A. Bueno -Orovio, and A. Banerjee, “Evaluating Convolution, Attention, and Mamba Based U -Net Models for Multi- class Bi -Atrial Segmentation from LGE-MRI,” in Lecture Notes in Computer Science, Springer Science and Business Media Deutschland GmbH, 2025, pp. 214–225. doi: 10.1007/978-3-031-87756-8_22
-
[11]
Multi-loss 3D Segmentation for Enhanced Bi- atrial Segmentation,
E. Almar-Munoz et al., “Multi-loss 3D Segmentation for Enhanced Bi- atrial Segmentation,” in Lecture Notes in Computer Science, Springer Science and Business Media Deutschland GmbH, 2025, pp. 236 –244. doi: 10.1007/978-3-031-87756-8_24
-
[12]
A. Zolotarev, K. Johnson, A. Khan, G. Slabaugh, and C. Roney, “An Ensemble of 3D Residual Encoder UNet Models for Solving Multi - class Bi-atrial Segmentation Challenge,” in Lecture Notes in Computer Science, Springer Science and Business Media Deutschland GmbH, 2025, pp. 209–213. doi: 10.1007/978-3-031-87756-8_21
-
[13]
A. M. Alsaleh, E. Albalawi, A. Algosaibi, S. S. Albakheet, and S. B. Khan, “Few-Shot Learning for Medical Image Segmentation Using 3D U-Net and Model -Agnostic Meta -Learning (MAML),” Diagnostics (Basel)., vol. 14, no. 12, Jun. 2024, doi: 10.3390/DIAGNOSTICS14121213
-
[14]
Meta-learning with implicit gradients in a few -shot setting for medical image segmentation,
R. Khadka et al., “Meta-learning with implicit gradients in a few -shot setting for medical image segmentation,” Comput. Biol. Med. , vol. 143, p. 105227, Apr. 2022, doi: 10.1016/J.COMPBIOMED.2022.105227
-
[15]
Few -shot Medical Image Segmentation with High- Fidelity Prototypes,
S. Tang et al. , “Few -shot Medical Image Segmentation with High- Fidelity Prototypes,” Med. Image Anal. , vol. 100, p. 103412, Feb. 2025, doi: 10.1016/J.MEDIA.2024.103412
-
[16]
Model-Agnostic Meta-Learning for Fast Adaptation of Deep Networks,
C. Finn, P. Abbeel, and S. Levine, “Model-Agnostic Meta-Learning for Fast Adaptation of Deep Networks,” Jul. 17, 2017, PMLR. Accessed: Jan. 13, 2026. [Online]. Available: https://proceedings.mlr.press/v70/finn17a.html
work page 2017
-
[17]
Learning to Segment Medical Images from Few -Shot Sparse Labels,
P. H. T. Gama, H. Oliveira, and J. A. Dos Santos, “Learning to Segment Medical Images from Few -Shot Sparse Labels,” SIBGRAPI Conference on Graphics, Patterns and Images , pp. 89 –96, 2021, doi: 10.1109/SIBGRAPI54419.2021.00021
-
[18]
Adaptive dynamic inference for few -shot left atrium segmentation,
J. Chen et al., “Adaptive dynamic inference for few -shot left atrium segmentation,” Med. Image Anal. , vol. 98, Dec. 2024, doi: 10.1016/j.media.2024.103321
-
[19]
Domain Adaptation for Medical Image Analysis: A Survey,
H. Guan and M. Liu, “Domain Adaptation for Medical Image Analysis: A Survey,” IEEE Trans. Biomed. Eng. , vol. 69, no. 3, p. 1173, Mar. 2022, doi: 10.1109/TBME.2021.3117407
-
[20]
Domain Generalization for Medical Image Analysis: A Review,
J. S. Yoon, K. Oh, Y. Shin, M. A. Mazurowski, and H. Il Suk, “Domain Generalization for Medical Image Analysis: A Review,” Proceedings of the IEEE , vol. 112, no. 10, pp. 1583 –1609, 2024, doi: 10.1109/JPROC.2024.3507831
-
[21]
A Survey on Domain Generalization for Medical Image Analysis,
Z. Niu, S. Ouyang, S. Xie, Y. Chen, and L. Lin, “A Survey on Domain Generalization for Medical Image Analysis,” Feb. 2024, Accessed: Jan. 13, 2026. [Online]. Available: https://arxiv.org/pdf/2402.05035v1
-
[22]
Z. Ye, K. Wang, W. Lv, Q. Feng, and L. Lu, “FSDA -DG: Improving Cross-Domain Generalizability of Medical Image Segmentation with Few Source Domain Annotations ,” Med. Image Anal. , vol. 105, p. 103704, Oct. 2025, doi: 10.1016/J.MEDIA.2025.103704
-
[23]
A. Raghu, M. Raghu, S. Bengio, and O. Vinyals, “Rapid Learning or Feature Reuse? Towards Understanding the Effectiveness of MAML,” 8th International Conference on Learning Representations, ICLR 2020, Sep. 2019, Accessed: Jan. 22, 2026. [Online]. Available: https://arxiv.org/pdf/1909.09157
-
[24]
On First-Order Meta-Learning Algorithms,
A. Nichol, J. Achiam, and J. Schulman, “On First-Order Meta-Learning Algorithms,” arXiv.org, 2018
work page 2018
-
[25]
O. Ronneberger, P. Fischer, and T. Brox, “U -Net: Convolutional Networks for Biomedical Image Segmentation,” Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), vol. 9351, pp. 234– 241, 2015, doi: 10.1007/978-3-319-24574-4_28
-
[26]
3D U -net: Learning dense volumetric segmentation from sparse annotation,
Ö. Çiçek, A. Abdulkadir, S. S. Lienkamp, T. Brox, and O. Ronneberger, “3D U -net: Learning dense volumetric segmentation from sparse annotation,” Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), vol. 9901 LNCS, pp. 424–432, 2016, doi: 10.1007/978-3-319-46723-8_49/TABLES/3
-
[27]
Boundary loss for highly unbalanced segmentation,
H. Kervadec, J. Bouchtiba, C. Desrosiers, E. Granger, J. Dolz, and I. Ben Ayed, “Boundary loss for highly unbalanced segmentation,” Med. Image Anal., vol. 67, Jan. 2021, doi: 10.1016/j.media.2020.101851
-
[28]
F. Isensee, P. F. Jaeger, S. A. A. Kohl, J. Petersen, and K. H. Maier - Hein, “nnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation,” Nature Methods 2020 18:2, vol. 18, no. 2, pp. 203–211, Dec. 2020, doi: 10.1038/s41592-020-01008-z
-
[29]
S. Nikolov et al. , “Clinically Applicable Segmentation of Head and Neck Anatomy for Radiotherapy: Deep Learning Algorithm Development and Validation Study,” J. Med. Internet Res., vol. 23, no. 7, Jul. 2021, doi: 10.2196/26151
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.