Recognition: 2 theorem links
· Lean TheoremUncertainty-Guided Latent Diagnostic Trajectory Learning for Sequential Clinical Diagnosis
Pith reviewed 2026-05-10 19:19 UTC · model grok-4.3
The pith
LLM agents learn latent diagnostic trajectories guided by uncertainty to enable better sequential clinical diagnosis.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
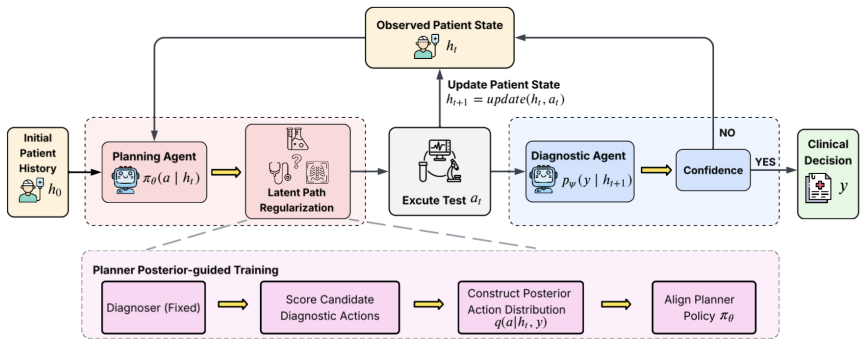
We introduce Latent Diagnostic Trajectory Learning (LDTL) as a framework consisting of a planning LLM agent and a diagnostic LLM agent. Diagnostic sequences are modeled as latent paths, and a posterior distribution is defined over them to prioritize those that provide greater diagnostic information. Training the planning agent to match this distribution produces coherent paths that progressively reduce uncertainty in the diagnosis process.
What carries the argument
The posterior distribution over latent diagnostic trajectories, which the planning LLM agent is trained to follow in order to reduce uncertainty step by step.
If this is right
- Diagnostic accuracy increases compared to prior methods.
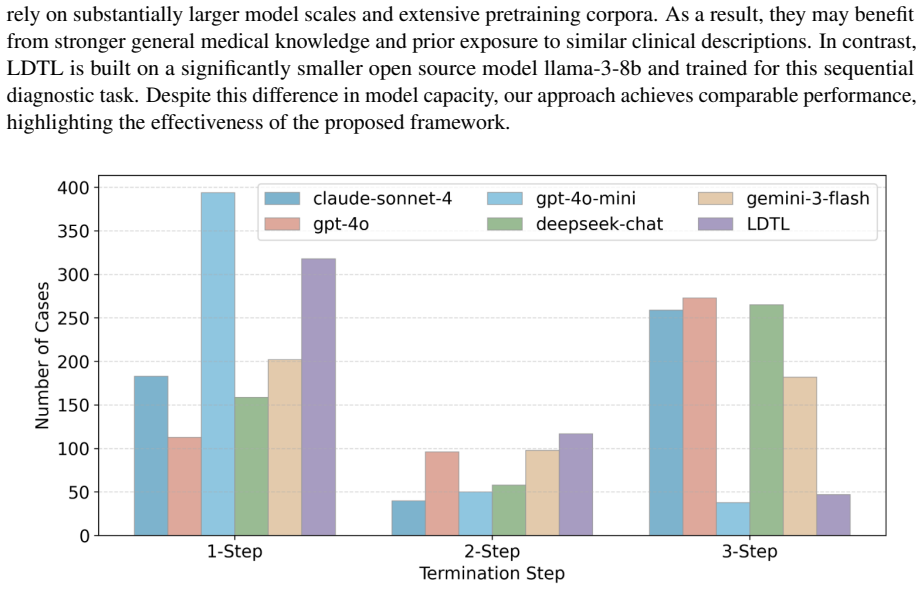
- The number of diagnostic tests ordered decreases.
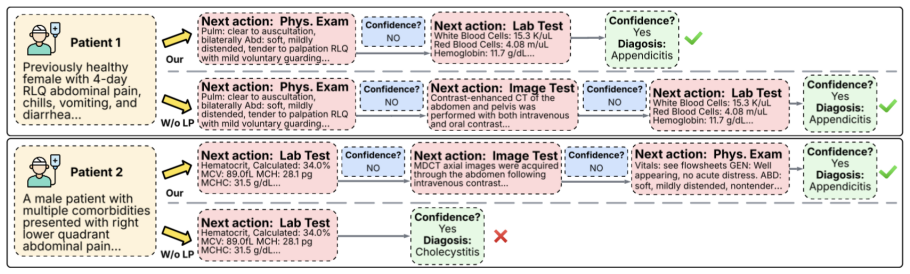
- Removing trajectory-level alignment reduces the performance gains.
- The framework works in settings where only final diagnoses are labeled, not the paths taken.
Where Pith is reading between the lines
- Similar latent-path training could help in other LLM planning scenarios that lack path supervision.
- The uncertainty reduction focus might connect to active learning methods in machine learning.
- Deployment in actual hospitals would require checking if the learned trajectories align with medical guidelines.
Load-bearing premise
It is possible to define and utilize a posterior distribution over diagnostic trajectories that effectively guides the planning agent without having explicit supervision for which paths are desirable in the data.
What would settle it
If the proposed LDTL framework does not achieve higher diagnostic accuracy or requires more tests than the best baselines when evaluated on the MIMIC-CDM benchmark, then the benefit of uncertainty-guided latent trajectory learning would not hold.
Figures


read the original abstract
Clinical diagnosis requires sequential evidence acquisition under uncertainty. However, most Large Language Model (LLM) based diagnostic systems assume fully observed patient information and therefore do not explicitly model how clinical evidence should be sequentially acquired over time. Even when diagnosis is formulated as a sequential decision process, it is still challenging to learn effective diagnostic trajectories. This is because the space of possible evidence-acquisition paths is relatively large, while clinical datasets rarely provide explicit supervision information for desirable diagnostic paths. To this end, we formulate sequential diagnosis as a Latent Diagnostic Trajectory Learning (LDTL) framework based on a planning LLM agent and a diagnostic LLM agent. For the diagnostic LLM agent, diagnostic action sequences are treated as latent paths and we introduce a posterior distribution that prioritizes trajectories providing more diagnostic information. The planning LLM agent is then trained to follow this distribution, encouraging coherent diagnostic trajectories that progressively reduce uncertainty. Experiments on the MIMIC-CDM benchmark demonstrate that our proposed LDTL framework outperforms existing baselines in diagnostic accuracy under a sequential clinical diagnosis setting, while requiring fewer diagnostic tests. Furthermore, ablation studies highlight the critical role of trajectory-level posterior alignment in achieving these improvements.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes the Latent Diagnostic Trajectory Learning (LDTL) framework for sequential clinical diagnosis with LLMs. It comprises a diagnostic LLM agent that models diagnostic action sequences as latent paths equipped with a posterior distribution over trajectories that prioritizes those providing more diagnostic information, and a planning LLM agent trained via alignment to this posterior to produce coherent paths that progressively reduce uncertainty. On the MIMIC-CDM benchmark the framework is reported to achieve higher diagnostic accuracy than baselines while using fewer tests; ablations are said to confirm the importance of the trajectory-level posterior alignment.
Significance. If the experimental results and the construction of the uncertainty-guided posterior hold under scrutiny, the work would provide a concrete mechanism for LLMs to handle the sequential, partially observed nature of clinical diagnosis without requiring explicit path-level supervision. This could reduce unnecessary diagnostic tests in clinical decision support while maintaining accuracy, addressing a practical gap in current LLM diagnostic systems. The approach of deriving a posterior from internal uncertainty estimates to guide planning is a potentially reusable idea for other sequential decision tasks lacking direct trajectory labels.
major comments (2)
- [§3.2] §3.2 (Posterior over latent trajectories): The posterior is defined to prioritize trajectories that supply more diagnostic information, yet the manuscript does not provide an independent, pre-specified measure of information gain or uncertainty reduction that is computed outside the training objective. Because MIMIC-CDM supplies no path-level labels, any circular dependence between the proxy used to define the posterior and the loss used to train the planning agent would undermine the claim that the learned trajectories are clinically preferable.
- [§4] §4 (Experiments on MIMIC-CDM): The headline claim that LDTL outperforms baselines in diagnostic accuracy while requiring fewer tests is not accompanied by the necessary reporting details—specific baseline methods, exact metrics (accuracy, test count, F1, etc.), statistical significance tests, confidence intervals, or the precise ablation isolating the posterior-alignment component. Without these, the central empirical result cannot be verified or reproduced.
minor comments (2)
- [Abstract] The abstract introduces the acronym LDTL without spelling it out on first use; this should be corrected for readability.
- [§3] Notation for the posterior p(·|·) and the uncertainty proxy should be introduced with explicit definitions and distinguished from the planning policy to avoid reader confusion.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive review. The comments highlight important areas for clarification and improved reporting, which we will address in the revision. Below we respond point-by-point to the major comments.
read point-by-point responses
-
Referee: [§3.2] §3.2 (Posterior over latent trajectories): The posterior is defined to prioritize trajectories that supply more diagnostic information, yet the manuscript does not provide an independent, pre-specified measure of information gain or uncertainty reduction that is computed outside the training objective. Because MIMIC-CDM supplies no path-level labels, any circular dependence between the proxy used to define the posterior and the loss used to train the planning agent would undermine the claim that the learned trajectories are clinically preferable.
Authors: We appreciate this observation on the construction of the posterior. In the LDTL framework, the posterior over latent diagnostic trajectories is defined using a fixed, pre-specified uncertainty measure: the Shannon entropy of the diagnostic LLM agent's predictive distribution over diagnoses, conditioned on the accumulated evidence at each step. This entropy is computed directly from the diagnostic agent's output logits and serves as an independent proxy for information gain; it does not depend on the planning agent's parameters or loss. The planning agent is subsequently trained via a separate alignment objective (KL divergence to the posterior) that encourages selection of trajectories reducing this entropy. While the current manuscript describes this process at a high level, we acknowledge that an explicit mathematical separation between the entropy computation and the alignment loss would strengthen the presentation and remove any perception of circularity. We will revise §3.2 to include the formal definition of the entropy-based information gain, a step-by-step derivation showing its independence from the planning loss, and a schematic diagram of the two-agent pipeline. This revision will also emphasize that the measure is clinically motivated (progressive uncertainty reduction) and fixed prior to training the planner. revision: yes
-
Referee: [§4] §4 (Experiments on MIMIC-CDM): The headline claim that LDTL outperforms baselines in diagnostic accuracy while requiring fewer tests is not accompanied by the necessary reporting details—specific baseline methods, exact metrics (accuracy, test count, F1, etc.), statistical significance tests, confidence intervals, or the precise ablation isolating the posterior-alignment component. Without these, the central empirical result cannot be verified or reproduced.
Authors: We agree that the experimental reporting in §4 must be expanded for reproducibility and verifiability. The revised manuscript will include: (i) an exhaustive list of all baseline methods with citations and implementation details; (ii) complete numerical results for accuracy, average diagnostic test count, F1-score, and any auxiliary metrics, reported as mean ± standard deviation over multiple random seeds; (iii) statistical significance tests (paired t-tests or Wilcoxon signed-rank tests) with p-values comparing LDTL against each baseline; (iv) 95% confidence intervals; and (v) a dedicated ablation table that isolates the trajectory-level posterior alignment component by comparing the full model against variants that omit the posterior or replace it with uniform sampling. We will also release the full codebase, hyperparameter settings, and evaluation scripts as supplementary material. These additions directly address the concerns about verification and will allow independent reproduction of the headline results. revision: yes
Circularity Check
No significant circularity detected in LDTL framework
full rationale
The paper defines a new LDTL framework by treating diagnostic sequences as latent paths and introducing a posterior over trajectories that prioritizes those providing more diagnostic information, then trains the planning agent to match this posterior. This is a constructive modeling choice to handle the absence of path-level supervision rather than a derivation that reduces by construction to its own inputs. No equations, fitted parameters renamed as predictions, or self-citation chains are shown that would force the central result. Performance claims rest on independent MIMIC-CDM benchmark experiments, which serve as external validation outside the framework definition itself.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption LLM agents can be trained to act as planners and diagnosticians over latent trajectories
invented entities (1)
-
Latent Diagnostic Trajectory
no independent evidence
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
we introduce a posterior distribution that prioritizes trajectories providing more diagnostic information... q(z|h0,y)=exp(βS(z))/∑exp(βS(z′))... approximated... IG(ht,a)=logp(y|ht+1)−logp(y|ht)... Lplanner=∑KL(q(a|ht,y)∥πθ(a|ht))
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
Experiments on the MIMIC-CDM benchmark demonstrate that our proposed LDTL framework outperforms existing baselines in diagnostic accuracy... while requiring fewer diagnostic tests.
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Variational inference: A review for statisti- cians.Journal of the American Statistical Associa- tion, 112(518):859–877. Tom B. Brown, Benjamin Mann, Nick Ryder, Melanie Subbiah, Jared Kaplan, Prafulla Dhariwal, Arvind Neelakantan, Pranav Shyam, Girish Sastry, Amanda Askell, Sandhini Agarwal, Ariel Herbert-V oss, Gretchen Krueger, Tom Henighan, Rewon Chil...
-
[2]
In Advances in Neural Information Processing Systems
Mediq: Question-asking llms and a bench- mark for reliable interactive clinical reasoning. In Advances in Neural Information Processing Systems. Hongcheng Liu, Yusheng Liao, Siqv Ou, Yuhao Wang, Heyang Liu, Yanfeng Wang, and Yu Wang. 2024. Med-pmc: Medical personalized multi-modal con- sultation with a proactive ask-first-observe-next paradigm.arXiv prepr...
-
[3]
V olodymyr Mnih, Koray Kavukcuoglu, David Silver, Andrei A
Towards accurate differential diagnosis with large language models.Nature, 642:451–457. V olodymyr Mnih, Koray Kavukcuoglu, David Silver, Andrei A. Rusu, Joel Veness, Marc G. Bellemare, Alex Graves, Martin Riedmiller, Andreas K. Fidje- land, Georg Ostrovski, and 1 others. 2015. Human- level control through deep reinforcement learning. Nature, 518(7540):52...
2015
-
[4]
Toolformer: Language Models Can Teach Themselves to Use Tools
Stochastic backpropagation and approximate inference in deep generative models.International Conference on Machine Learning. Timo Schick, Jane Dwivedi-Yu, Roberto Dessì, Roberta Raileanu, Maria Lomeli, Luke Zettlemoyer, Nicola Cancedda, and Thomas Scialom. 2023. Toolformer: Language models can teach themselves to use tools. arXiv preprint arXiv:2302.04761...
work page internal anchor Pith review arXiv 2023
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.