Recognition: 1 theorem link
· Lean TheoremPredicting Alzheimer's disease progression using rs-fMRI and a history-aware graph neural network
Pith reviewed 2026-05-10 18:38 UTC · model grok-4.3
The pith
A history-aware graph neural network predicts Alzheimer's stage transitions from rs-fMRI at 82.9% accuracy.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The authors claim that a GNN model equipped with an RNN block can process an entire history of rs-fMRI-derived functional connectivity graphs, incorporate visit-distance features, and output the next cognitive stage for each subject, achieving 82.9% accuracy across CN, MCI, and AD transitions on 303 subjects and 68.8% accuracy specifically on CN-to-MCI conversions, while remaining robust when some visits are absent.
What carries the argument
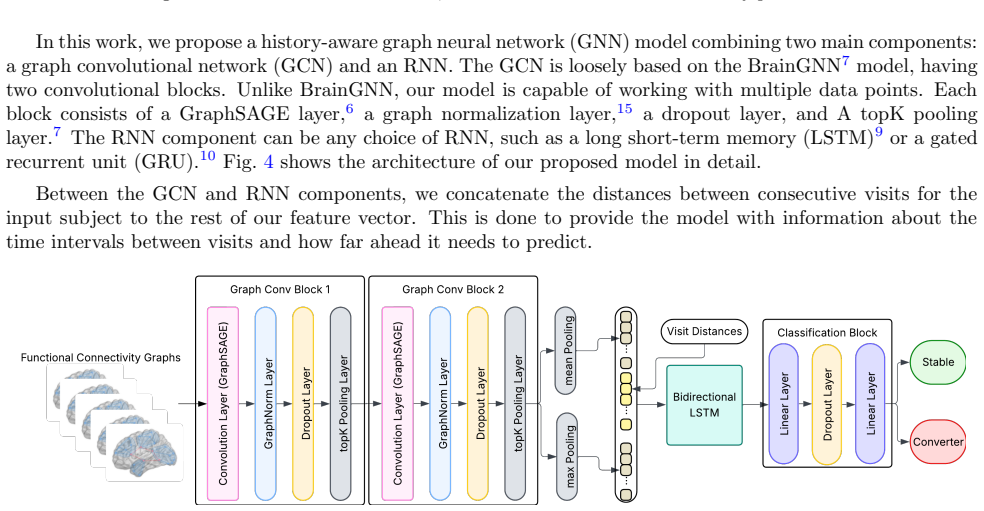
A graph neural network whose message-passing layers receive functional connectivity graphs from each rs-fMRI visit and whose output is sequenced by an RNN block that also receives explicit visit-interval values, allowing the network to model longitudinal progression.
If this is right
- Timely prediction of CN-to-MCI transitions could allow interventions before full AD develops.
- The model continues to function when visits are irregularly spaced or partially missing, matching typical clinical data.
- rs-fMRI functional connectivity alone supplies usable information for forecasting MCI or AD onset.
- The same architecture could be combined with other modalities to raise accuracy further.
Where Pith is reading between the lines
- If the same graph-plus-history structure works on larger or multi-site data, the method could support population-level screening programs.
- The robustness to missing visits opens the possibility of applying the model to retrospective medical records that lack complete follow-up.
- Architectures that fuse GNNs on brain graphs with RNNs on time sequences may transfer to progression modeling in other neurodegenerative conditions.
Load-bearing premise
The functional connectivity graphs extracted from rs-fMRI plus the sequence of visit times contain enough generalizable signal to forecast future stage changes without being tied to the particular 303-subject cohort or requiring dataset-specific fixes.
What would settle it
Train the model on the reported 303-subject set and then test it unchanged on an independent external cohort that supplies rs-fMRI scans, visit dates, and confirmed stage labels at the subsequent visit; accuracy below 70% on the full task or below 60% on CN-to-MCI would falsify the claim.
Figures




read the original abstract
Alzheimer's disease (AD) is a neurodegenerative disorder that affects more than seven million people in the United States alone. AD currently has no cure, but there are ways to potentially slow its progression if caught early enough. In this study, we propose a graph neural network (GNN)-based model for predicting whether a subject will transition to a more severe stage of cognitive impairment at their next clinical visit. We consider three stages of cognitive impairment in order of severity: cognitively normal (CN), mild cognitive impairment (MCI), and AD. We use functional connectivity graphs derived from resting-state functional magnetic resonance imaging (rs-fMRI) scans of 303 subjects, each with a different number of visits. Our GNN-based model incorporates a recurrent neural network (RNN) block, enabling it to process data from the subject's entire visit history. It can also work with irregular time gaps between visits by incorporating visit distance information into our input features. Our model demonstrates robust predictive performance, even with missing visits in the subjects' visit histories. It achieves an accuracy of 82.9%, with an especially impressive accuracy of 68.8% on CN to MCI conversions - a task that poses a substantial challenge in the field. Our results highlight the effectiveness of rs-fMRI in predicting the onset of MCI or AD and, in conjunction with other modalities, could offer a viable method for enabling timely interventions to slow the progression of cognitive impairment.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes a GNN model augmented with an RNN block to predict transitions between cognitive stages (CN, MCI, AD) from rs-fMRI functional connectivity graphs. It processes longitudinal visit histories with irregular intervals and missing data for a cohort of 303 subjects, reporting 82.9% overall accuracy and 68.8% accuracy specifically on CN-to-MCI conversions.
Significance. If the performance holds under proper validation, the history-aware architecture offers a practical way to leverage rs-fMRI for early detection of progression, addressing a clinically relevant gap where CN-to-MCI prediction is difficult. The explicit handling of visit timing and missing data is a constructive modeling choice for real-world longitudinal cohorts.
major comments (2)
- Abstract: The reported accuracies (82.9% overall, 68.8% on CN-to-MCI) are presented without any information on validation splits, subject-independent cross-validation, class balance, statistical tests, or handling of missing visits. With only 303 subjects and infrequent conversion events, this absence directly undermines assessment of whether the numbers reflect generalizable signals or cohort-specific overfitting.
- Methods/Results (inferred from abstract claims): The central assertion that rs-fMRI graphs plus RNN-processed history suffice for robust prediction lacks supporting details on baseline comparisons, ablation of the RNN or visit-distance features, or external test-set performance. Without these, the 68.8% CN-to-MCI figure cannot be evaluated as evidence of predictive utility rather than leakage or post-hoc tuning.
minor comments (1)
- Abstract: Provide the number of subjects per diagnostic category and the observed conversion rates to allow readers to interpret the reported accuracies in context.
Simulated Author's Rebuttal
We thank the referee for the constructive comments, which identify key areas where additional details will strengthen the manuscript's clarity and rigor. We address each major comment below and will incorporate the suggested revisions.
read point-by-point responses
-
Referee: Abstract: The reported accuracies (82.9% overall, 68.8% on CN-to-MCI) are presented without any information on validation splits, subject-independent cross-validation, class balance, statistical tests, or handling of missing visits. With only 303 subjects and infrequent conversion events, this absence directly undermines assessment of whether the numbers reflect generalizable signals or cohort-specific overfitting.
Authors: We agree that the abstract and main text require more explicit details on the validation protocol to support the reported performance. In the revised manuscript, we will expand the abstract and Methods section to describe the subject-independent cross-validation procedure, how class imbalance was addressed (via weighted loss functions given the rarity of conversions), the statistical tests applied (e.g., McNemar's test or bootstrap confidence intervals), and the specific mechanisms for handling missing visits and irregular intervals. We will also report cohort statistics on conversion event frequency and discuss potential overfitting risks in light of the sample size of 303 subjects, ensuring readers can better evaluate generalizability. revision: yes
-
Referee: Methods/Results (inferred from abstract claims): The central assertion that rs-fMRI graphs plus RNN-processed history suffice for robust prediction lacks supporting details on baseline comparisons, ablation of the RNN or visit-distance features, or external test-set performance. Without these, the 68.8% CN-to-MCI figure cannot be evaluated as evidence of predictive utility rather than leakage or post-hoc tuning.
Authors: We acknowledge that baseline comparisons and ablations are essential to isolate the contributions of the history-aware components. In the revised manuscript, we will add a dedicated ablation study section comparing the full model against (i) a standard GNN without the RNN block, (ii) a version without visit-distance features, and (iii) non-graph baselines such as SVMs or LSTMs on vectorized features. We will also clarify the cross-validation design (subject-independent folds to avoid leakage) and discuss the absence of a fully held-out external test set due to the single-cohort nature of the data, while providing internal validation metrics with confidence intervals. These additions will allow direct assessment of whether the 68.8% CN-to-MCI accuracy reflects genuine predictive utility. revision: yes
Circularity Check
Empirical ML evaluation on cohort data shows no circularity
full rationale
The paper presents a GNN model augmented with an RNN block to process subject visit histories from rs-fMRI functional connectivity graphs, reporting empirical accuracies of 82.9% overall and 68.8% on CN-to-MCI transitions after training and evaluation on the 303-subject dataset. No mathematical derivations, equations, uniqueness theorems, or self-citations are invoked that reduce the reported performance metrics to quantities defined by construction from fitted parameters or prior author results. The central claims rest on standard supervised learning outcomes rather than any self-referential reduction, making the work self-contained as an empirical study.
Axiom & Free-Parameter Ledger
free parameters (1)
- GNN and RNN architecture hyperparameters
axioms (2)
- domain assumption Functional connectivity graphs derived from rs-fMRI contain information predictive of future cognitive stage transitions
- domain assumption Incorporating visit history via RNN improves prediction over single-scan models
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclearOur GNN-based model incorporates a recurrent neural network (RNN) block... functional connectivity graphs derived from rs-fMRI... 303 subjects... accuracy of 82.9%
Reference graph
Works this paper leans on
-
[1]
Alzheimer’s disease,
Scheltens, P., Blennow, K., Breteler, M. M. B., de Strooper, B., Frisoni, G. B., Salloway, S., and Van der Flier, W. M., “Alzheimer’s disease,”The Lancet388(10043), 505–517 (2016)
2016
-
[2]
Dementia prevention, intervention, and care: 2020 report of the lancet commission,
Livingston, G., Huntley, J., Sommerlad, A., Ames, D., Ballard, C., Banerjee, S., Brayne, C., Burns, A., Cohen-Mansfield, J., Cooper, C., Costafreda, S. G., Dias, A., Fox, N., Gitlin, L. N., Howard, R., Kales, H. C., Kivim¨ aki, M., Larson, E. B., Ogunniyi, A., Orgeta, V., Ritchie, K., Rockwood, K., Sampson, E. L., Samus, Q., Schneider, L. S., Selbæk, G., ...
2020
-
[3]
The alzheimer’s disease neuroimaging initiative (adni): Mri methods,
Jack, C. R., Bernstein, M. A., Fox, N. C., Thompson, P. M., Alexander, G. E., Harvey, D. J., Borowski, B. J., Britson, P. J., Whitwell, J. L., Ward, C. P., Dale, A. M., Felmlee, J. P., Gunter, J. L., Hill, D. L. G., Killiany, R. J., Schuff, N., Fox-Bosetti, S., Lin, C., Studholme, C., DeCarli, C., Krueger, G., Ward, H. A., Metzger, G. J., Scott, K. T., Ma...
2008
-
[4]
The role of neuroimag- ing in alzheimer’s disease: implications for the diagnosis, monitoring disease progression, and treatment,
Mulumba, J., Duan, R., Luo, B., Wu, J., Sulaiman, M., Wang, F., and Yang, Y., “The role of neuroimag- ing in alzheimer’s disease: implications for the diagnosis, monitoring disease progression, and treatment,” Exploration of Neuroscience4(Feb. 2025)
2025
-
[5]
Brain inflammation, degeneration, and plasticity in multiple sclerosis,
Granziera, C. and Sprenger, T., “Brain inflammation, degeneration, and plasticity in multiple sclerosis,” in [Brain Mapping], Toga, A. W., ed., 917–927, Academic Press, Waltham (2015)
2015
-
[6]
Inductive Representation Learning on Large Graphs
Hamilton, W. L., Ying, Z., and Leskovec, J., “Inductive representation learning on large graphs,” ArXivabs/1706.02216(2017)
work page Pith review arXiv 2017
-
[7]
Braingnn: Interpretable brain graph neural network for fmri analysis,
Li, X., Zhou, Y., Gao, S., Dvornek, N. C., Zhang, M., Zhuang, J., Gu, S., Scheinost, D., Staib, L. H., Ventola, P., and Duncan, J. S., “Braingnn: Interpretable brain graph neural network for fmri analysis,” bioRxiv(2020)
2020
-
[8]
Transformer model for alzheimer’s disease progression prediction using longitudinal visit sequences,
Moghaddami, M., Schubring, C., and Siadat, M., “Transformer model for alzheimer’s disease progression prediction using longitudinal visit sequences,” in [Proceedings of the sixth Conference on Health, Inference, and Learning], Xu, X. O., Choi, E., Singhal, P., Gerych, W., Tang, S., Agrawal, M., Subbaswamy, A., Sizikova, E., Dunn, J., Daneshjou, R., Sarker...
2025
-
[9]
Long short-term memory,
Hochreiter, S. and Schmidhuber, J., “Long short-term memory,”Neural computation9(8), 1735–1780 (1997)
1997
-
[10]
Learning phrase representations using rnn encoder–decoder for statistical machine translation,
Cho, K., van Merrienboer, B., C ¸ aglar G¨ ul¸ cehre, Bahdanau, D., Bougares, F., Schwenk, H., and Bengio, Y., “Learning phrase representations using rnn encoder–decoder for statistical machine translation,” in [Conference on Empirical Methods in Natural Language Processing], (2014)
2014
-
[11]
Tadpole challenge: Prediction of longitudinal evolution in alzheimer’s disease.,
Marinescu, R. V., Oxtoby, N. P., Young, A. L., Bron, E., Toga, A. W., Weiner, M. W., Barkhof, F., Fox, N. C., Klein, S., Alexander, D. C., the EuroPOND Consortium, and the Alzheimer’s Disease Neuroimag- ing Initiative, F., “Tadpole challenge: Prediction of longitudinal evolution in alzheimer’s disease.,”arXiv: Populations and Evolution(2018)
2018
-
[12]
fmriprep: a robust preprocessing pipeline for functional mri,
Esteban, O., Markiewicz, C. J., Blair, R. W., Moodie, C. A., Isik, A. I., Erramuzpe, A., Kent, J. D., Goncalves, M., DuPre, E., Snyder, M., Oya, H., Ghosh, S. S., Wright, J., Durnez, J., Poldrack, R. A., and Gorgolewski, K. J., “fmriprep: a robust preprocessing pipeline for functional mri,”Nature Methods16, 111–116 (Dec. 2018)
2018
-
[13]
The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments,
Gorgolewski, K. J., Auer, T., Calhoun, V. D., Craddock, R. C., Das, S., Duff, E. P., Flandin, G., Ghosh, S. S., Glatard, T., Halchenko, Y. O., Handwerker, D. A., Hanke, M., Keator, D. B., Li, X., Michael, Z., Maumet, C., Nichols, B. N., Nichols, T. E., Pellman, J., Poline, J.-B., Rokem, A. S., Schaefer, G., Sochat, V. V., Triplett, W., Turner, J. A., Varo...
2016
-
[14]
Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity mri,
Schaefer, A., Kong, R., Gordon, E. M., Laumann, T. O., Zuo, X.-N., Holmes, A. J., Eickhoff, S. B., and Yeo, B. T. T., “Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity mri,”Cerebral Cortex28, 3095–3114 (July 2017)
2017
-
[15]
Graphnorm: A principled approach to accelerating graph neural network training,
Cai, T., Luo, S., Xu, K., He, D., Liu, T.-Y., and Wang, L., “Graphnorm: A principled approach to accelerating graph neural network training,” in [International Conference on Machine Learning], (2020)
2020
-
[16]
Practical bayesian optimization of machine learning algo- rithms,
Snoek, J., Larochelle, H., and Adams, R. P., “Practical bayesian optimization of machine learning algo- rithms,” in [Proceedings of the 26th International Conference on Neural Information Processing Systems - Volume 2],NIPS’12, 2951–2959, Curran Associates Inc., Red Hook, NY, USA (2012)
2012
-
[17]
Focal loss for dense object detection,
Lin, T.-Y., Goyal, P., Girshick, R. B., He, K., and Doll´ ar, P., “Focal loss for dense object detection,”2017 IEEE International Conference on Computer Vision (ICCV), 2999–3007 (2017)
2017
-
[18]
The use of the area under the roc curve in the evaluation of machine learning algorithms,
Bradley, A. P., “The use of the area under the roc curve in the evaluation of machine learning algorithms,” Pattern Recognit.30, 1145–1159 (1997)
1997
-
[19]
Interpretable temporal graph neural network for prognostic prediction of alzheimer’s disease using longitudinal neuroimaging data,
Kim, M., Kim, J., Qu, J., Huang, H., Long, Q., Sohn, K.-A., Kim, D., and Shen, L., “Interpretable temporal graph neural network for prognostic prediction of alzheimer’s disease using longitudinal neuroimaging data,” in [2021 IEEE International Conference on Bioinformatics and Biomedicine (BIBM)], 1381–1384, IEEE (Dec. 2021)
2021
-
[20]
Predicting the conversion from mild cognitive impairment to alzheimer’s disease using an explainable ai approach,
Grammenos, G., Vrahatis, A. G., Vlamos, P., Palejev, D., and Exarchos, T., “Predicting the conversion from mild cognitive impairment to alzheimer’s disease using an explainable ai approach,”Information15, 249 (Apr. 2024)
2024
-
[21]
A self-guided multimodal approach to enhancing graph representation learning for alzheimer’s diseases,
Wang, Z., Bao, R., Wu, Y., Liu, G., Yang, L., Zhan, L., Zheng, F., Jiang, W., and Zhang, Y., “A self-guided multimodal approach to enhancing graph representation learning for alzheimer’s diseases,” (2024)
2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.