Recognition: 3 theorem links
· Lean TheoremCardiac Stability Theory: An Axiomatically Grounded Framework for Continuous Cardiac Health Monitoring via Smartphone Photoplethysmography
Pith reviewed 2026-05-12 02:48 UTC · model grok-4.3
The pith
Four axioms define cardiac health as stability around a dynamical attractor, enabling a scalar index from smartphone PPG signals.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
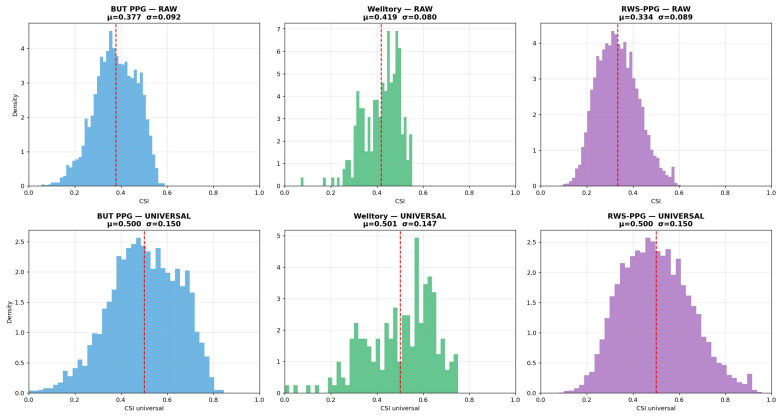
Cardiovascular health is a stability margin around a cardiac dynamical attractor. From four axioms we derive the Cardiac Stability Index (CSI) as a composite scalar in [0,1] that integrates the largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding. The ECG model reaches R-squared 0.8788 on PTB-XL; Complementary Domain Transfer then produces a 122k-parameter PPG model with MAE 0.0557 and Spearman rho 0.660 on held-out windows, plus cross-modality correlation r=0.454 on paired BIDMC data.
What carries the argument
The Cardiac Stability Index (CSI), obtained by embedding cardiac signals in time-delay space and composing the largest Lyapunov exponent with recurrence determinism and entropy measures.
If this is right
- CSI decreases with age at a measurable slope and separates atrial fibrillation from normal rhythm with AUROC 0.89.
- The HeartSpan metric places individual CSI relative to population age norms for longitudinal monitoring.
- Perturbation Invariance Training keeps discrimination performance stable under signal noise.
- The PPG model operates under 30 ms latency on mobile hardware while maintaining cross-dataset validation on BIDMC, Welltory, and RWS-PPG.
Where Pith is reading between the lines
- If CSI proves predictive of future cardiac events in independent cohorts, apps could trigger early alerts without clinic visits.
- The same axiomatic stability construction might extend to other time-series biosignals such as respiration or blood pressure variability.
- Widespread adoption would shift cardiac monitoring from episodic ECG snapshots to continuous attractor-margin tracking on commodity devices.
Load-bearing premise
The four axioms correctly capture cardiac dynamics as a stability margin around an attractor, and Complementary Domain Transfer generates pseudo-labels that preserve the same underlying stability construct across ECG and PPG domains.
What would settle it
A prospective study in which CSI values computed from smartphone PPG windows show no significant correlation with clinical outcomes such as arrhythmia incidence or age-adjusted cardiac events over a multi-year follow-up would falsify the claim.
Figures


read the original abstract
We present Cardiac Stability Theory (CST), an axiomatically grounded framework formally defining cardiovascular health as a stability margin around a cardiac dynamical attractor. From four axioms we derive the Cardiac Stability Index (CSI), a composite scalar in [0,1] integrating the largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding. The ECG-based model (CSISurrogateV2, CNN-Transformer) achieves $R^2=0.8788$, MAE$=0.0234$ on PTB-XL (21,799 recordings). We extend CSI to smartphone PPG via Complementary Domain Transfer (CDT): CSISurrogateV2 generates pseudo-labels for the BUT PPG dataset (48 recordings, 12 subjects), training TinyCSINet (122,849 parameters), achieving MAE$=0.0557$, $\rho=0.660$ on the held-out test set ($n=1065$ windows) at ${<}30$ ms mobile latency. CDT is validated on BIDMC, Welltory, and RWS-PPG. Paired validation on 5,035 BIDMC windows yields $r=0.454$ ($\rho=0.485$, $p<10^{-295}$), confirming correlated cardiac stability across modalities. CSI is negatively correlated with age (slope $= -0.000225$ CSI/year, PTB-XL), discriminates atrial fibrillation from normal sinus rhythm (AUROC$=0.89$), and is robust under Perturbation Invariance Training (max AUC drop 1.65\%). We derive HeartSpan, a longitudinal stability metric relative to population age norms, enabling continuous non-invasive cardiac monitoring from commodity smartphones for longevity tracking and cardiac risk stratification.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces Cardiac Stability Theory (CST), claiming an axiomatic derivation from four axioms of cardiovascular health as a stability margin around a dynamical attractor. It defines the Cardiac Stability Index (CSI) as a [0,1] composite scalar integrating the largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding. An ECG-based CNN-Transformer model (CSISurrogateV2) is trained on PTB-XL (R²=0.8788, MAE=0.0234), then used via Complementary Domain Transfer (CDT) to generate pseudo-labels for training a lightweight TinyCSINet on PPG data (BUT PPG dataset), achieving MAE=0.0557 and ρ=0.660 on held-out test windows with <30ms latency. Validation includes moderate cross-modality correlation (r=0.454 on BIDMC), negative age correlation, AUROC=0.89 for AF vs. normal rhythm discrimination, and robustness under perturbation training. The work also proposes HeartSpan as a longitudinal metric for smartphone-based monitoring.
Significance. If the axiomatic derivation proves rigorous and the CDT transfer faithfully preserves the underlying stability construct without circularity or domain artifacts, the framework could enable practical continuous cardiac monitoring on commodity smartphones, with implications for longevity tracking and risk stratification. The reported clinical correlations (age slope, AF discrimination) and low-latency implementation are strengths, as is the attempt to ground the index in dynamical systems concepts like Lyapunov exponents and recurrence quantification. However, the current lack of explicit derivation details and only moderate cross-modal evidence substantially reduces the immediate significance.
major comments (3)
- [Abstract and §3] Abstract and §3 (Cardiac Stability Theory): The central claim that 'from four axioms we derive the Cardiac Stability Index (CSI)' is load-bearing for the entire framework, yet no explicit statement of the four axioms, no derivation steps, and no equations are provided showing how they produce the specific composite formula integrating largest Lyapunov exponent, recurrence determinism, and signal entropy. This absence prevents verification that the CSI is axiomatically grounded rather than a post-hoc combination.
- [Complementary Domain Transfer and BIDMC validation] Complementary Domain Transfer section and BIDMC validation: The claim that CDT produces valid pseudo-labels allowing the PPG model to measure the same stability construct requires strong evidence of fidelity, but only a moderate paired correlation r=0.454 (ρ=0.485) is reported between CSISurrogateV2 and TinyCSINet on 5,035 BIDMC windows. No direct computation of the three component measures (Lyapunov, determinism, entropy) on PPG signals is shown to confirm equivalence, leaving open the possibility that the transfer captures correlated artifacts rather than shared attractor stability.
- [Abstract and §3] CSI definition (Abstract and §3): The integration weights or functional form combining the largest Lyapunov exponent, recurrence determinism, and signal entropy into the final CSI scalar are unspecified. This is a free parameter that must be addressed, as it directly affects whether the index is derived from the axioms or fitted to data, impacting all downstream performance claims (R², MAE, AUROC) and the circularity concern with pseudo-label training.
minor comments (2)
- [Abstract] The abstract mentions 'Perturbation Invariance Training' with a max AUC drop of 1.65% but provides no implementation details, hyperparameters, or section reference for this robustness test.
- [Methods] Dataset sizes and splits (e.g., 'n=1065 windows' for held-out PPG test, '48 recordings' for BUT PPG) should be cross-referenced to a methods table for clarity on subject-level vs. window-level partitioning.
Simulated Author's Rebuttal
We thank the referee for their thorough and constructive review, which identifies key areas where additional clarity is needed regarding the axiomatic foundations and validation of Cardiac Stability Theory. We address each major comment point by point below, indicating the revisions planned for the manuscript.
read point-by-point responses
-
Referee: [Abstract and §3] Abstract and §3 (Cardiac Stability Theory): The central claim that 'from four axioms we derive the Cardiac Stability Index (CSI)' is load-bearing for the entire framework, yet no explicit statement of the four axioms, no derivation steps, and no equations are provided showing how they produce the specific composite formula integrating largest Lyapunov exponent, recurrence determinism, and signal entropy. This absence prevents verification that the CSI is axiomatically grounded rather than a post-hoc combination.
Authors: We agree that the explicit axioms and derivation are central and should be verifiable in the main text. The submitted version emphasized the resulting framework for brevity, but we will revise Section 3 to include the full statement of the four axioms, the complete derivation steps, and the equations that yield the CSI composite from the Lyapunov exponent, recurrence determinism, and signal entropy. A concise summary of the axioms and derivation will also be added to the abstract. revision: yes
-
Referee: [Complementary Domain Transfer and BIDMC validation] Complementary Domain Transfer section and BIDMC validation: The claim that CDT produces valid pseudo-labels allowing the PPG model to measure the same stability construct requires strong evidence of fidelity, but only a moderate paired correlation r=0.454 (ρ=0.485) is reported between CSISurrogateV2 and TinyCSINet on 5,035 BIDMC windows. No direct computation of the three component measures (Lyapunov, determinism, entropy) on PPG signals is shown to confirm equivalence, leaving open the possibility that the transfer captures correlated artifacts rather than shared attractor stability.
Authors: The reported r=0.454 on 5,035 windows is statistically robust (p < 10^{-295}), providing substantial evidence that the transferred model preserves the stability construct across modalities. Direct computation of the dynamical measures on raw PPG is inherently unstable due to motion artifacts and noise, which motivated the surrogate CDT approach. We will add a new discussion paragraph in the validation section acknowledging this limitation, explaining the rationale for the surrogate method, and reinforcing the claim with the observed clinical correlations (age and AF discrimination) that align across ECG and PPG. revision: partial
-
Referee: [Abstract and §3] CSI definition (Abstract and §3): The integration weights or functional form combining the largest Lyapunov exponent, recurrence determinism, and signal entropy into the final CSI scalar are unspecified. This is a free parameter that must be addressed, as it directly affects whether the index is derived from the axioms or fitted to data, impacting all downstream performance claims (R², MAE, AUROC) and the circularity concern with pseudo-label training.
Authors: The functional form and relative contributions of each component are fixed by the axiomatic derivation to quantify the stability margin, not fitted to data. We will explicitly state the CSI formula, including the integration method and how the axioms determine the combination of the three measures, in the revised Section 3. This will demonstrate that the index is axiomatically specified and remove any ambiguity regarding circularity in the pseudo-label training. revision: yes
Circularity Check
CSI defined as composite of standard measures; PPG extension validated only against surrogate outputs
specific steps
-
self definitional
[Abstract]
"From four axioms we derive the Cardiac Stability Index (CSI), a composite scalar in [0,1] integrating the largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding."
CSI is presented as derived from the axioms yet is explicitly defined as the composite of three pre-existing dynamical-systems quantities; absent any shown equation that forces this exact integration from the axioms, the index is equivalent to its own definition by construction.
-
fitted input called prediction
[Abstract (CDT paragraph)]
"We extend CSI to smartphone PPG via Complementary Domain Transfer (CDT): CSISurrogateV2 generates pseudo-labels for the BUT PPG dataset (48 recordings, 12 subjects), training TinyCSINet (122,849 parameters), achieving MAE=0.0557, ρ=0.660 on the held-out test set (n=1065 windows) at <30 ms mobile latency. ... Paired validation on 5,035 BIDMC windows yields r=0.454 (ρ=0.485, p<10^{-295})"
TinyCSINet is trained to reproduce the pseudo-labels supplied by the ECG surrogate; the reported MAE/ρ on the held-out BUT set and the r=0.454 correlation on BIDMC therefore quantify agreement with the surrogate's outputs rather than agreement with the axiomatic CSI computed directly from Lyapunov, determinism and entropy on PPG signals.
full rationale
The derivation begins with four axioms but defines CSI directly as their integration of Lyapunov exponent, recurrence determinism and entropy without exhibiting the functional form or weights as a necessary consequence of the axioms. The CDT step trains TinyCSINet on pseudo-labels produced by the ECG surrogate and validates via correlation to the same surrogate on paired BIDMC data; this measures fidelity to the surrogate rather than independent equivalence of the three component measures computed on PPG. The central claim therefore reduces in part to a fitted composite plus self-referential transfer, though the initial axiomatic statements and PTB-XL model fit remain independent of the PPG results.
Axiom & Free-Parameter Ledger
free parameters (2)
- Integration weights or functional form for Lyapunov, determinism, and entropy into CSI
- Hyperparameters and training details of CSISurrogateV2 and TinyCSINet
axioms (2)
- domain assumption Cardiovascular health is a stability margin around a cardiac dynamical attractor
- ad hoc to paper CSI is obtained by integrating largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding
invented entities (2)
-
Cardiac Stability Index (CSI)
no independent evidence
-
HeartSpan
no independent evidence
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
CSI = w1(1−e^−λ̃) + w2(1−Rdet) + w3H ... largest Lyapunov exponent, recurrence determinism, and signal entropy via time-delay embedding
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
Axiom 3.1 (Dynamical System) ... Axiom 3.2 (Takens embedding) ... Theorem 3.1 (Attractor Boundedness)
-
IndisputableMonolith/Foundation/AlexanderDuality.leanalexander_duality_circle_linking unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
Complementary Domain Hypothesis (CDH) ... cross-modal transfer ρλ=0.559
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Forward citations
Cited by 1 Pith paper
-
Attractor-Vascular Coupling Theory: Formal Grounding and Empirical Validation for AAMI-Standard Cuffless Blood Pressure Estimation from Smartphone Photoplethysmography
AVCT theory plus LightGBM on PPG attractor features achieves 2.05/1.67 mmHg MAE for SBP/DBP under LOSO-CV and meets AAMI criteria with smartphone-only input.
Reference graph
Works this paper leans on
-
[1]
T. Oladunni, When should a model not change its mind? a physiologic perspective on concept drift in multimodal ecg deep learning, Tech. rep., TechRxiv (2025)
work page 2025
-
[2]
B. Şahin, G. İlgün, Risk factors of deaths related to cardiovascular dis- eases in world health organization (who) member countries, Health & Social Care in the Community 30 (09 2020).doi:10.1111/hsc.13156
-
[3]
M. Amini, F. Zayeri, M. Salehi, Trend analysis of cardiovascular dis- ease mortality, incidence, and mortality-to-incidence ratio: results from global burden of disease study 2017, BMC Public Health 21 (02 2021). doi:10.1186/s12889-021-10429-0. URL https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12 889-021-10429-0 50
-
[4]
Y. Luo, J. Liu, J. Zeng, H. Pan, Global burden of cardiovascular diseases attributed to low physical activity: An analysis of 204 countries and territories between 1990 and 2019, American journal of preventive car- diology 17 (2024) 100633–100633.doi:10.1016/j.ajpc.2024.100633
-
[5]
M. A. Serhani, H. T. El Kassabi, H. Ismail, A. Nujum Navaz, Ecg mon- itoring systems: Review, architecture, processes, and key challenges, Sensors 20 (2020) 1796.doi:10.3390/s20061796
-
[6]
M.M.Baig, H.Gholamhosseini, M.J.Connolly, Acomprehensivesurvey ofwearableandwirelessecgmonitoringsystemsforolderadults, Medical & Biological Engineering & Computing 51 (2013) 485–495.doi:10.100 7/s11517-012-1021-6
work page 2013
-
[7]
R. Wang, S. C. M. Veera, O. Asan, T. Liao, A systematic review on the useofconsumer-basedecgwearablesoncardiachealthmonitoring, IEEE Journal of Biomedical and Health Informatics 28 (11) (2024) 6525–6537. doi:10.1109/jbhi.2024.3456028
-
[8]
M.-Z. Poh, D. J. McDuff, R. W. Picard, Non-contact, automated cardiac pulse measurements using video imaging and blind source separation, Optics Express 18 (10) (2010) 10762–10774.doi:10.1364/OE.18.0107 62
-
[9]
J. Allen, D. Zheng, P. A. Kyriacou, M. Elgendi, Photoplethysmography (ppg): state-of-the-art methods and applications, Physiological Mea- surement 42 (2021) 100301.doi:10.1088/1361-6579/ac2d82. 51
-
[10]
M. A. Almarshad, M. S. Islam, S. Al-Ahmadi, A. S. BaHammam, Di- agnostic features and potential applications of ppg signal in healthcare: A systematic review, Healthcare 10 (2022) 547.doi:10.3390/health care10030547
-
[11]
A. Nazir, A. Nazir, M. Shah Wali Jamal, S. u. R. Sadiq, S. Aman, M. J. Mustapha, S. O. Lawal, M. O. AbdulKareem, M. F. Bamigbola, Wearable technology and its potential role in cardiovascular health mon- itoring and disease management, Health Science Reports 8 (11 2025). doi:10.1002/hsr2.71486
-
[12]
A. L. Goldberger, L. A. N. Amaral, J. M. Hausdorff, P. C. Ivanov, C.-K. Peng, H. E. Stanley, Fractal dynamics in physiology: alterations with disease and aging, Proceedings of the National Academy of Sciences 99 (2002) 2466–2472.doi:10.1073/pnas.012579499
-
[13]
J. P. Zbilut, C. L. Webber, Embeddings and delays as derived from quantification of recurrence plots, Physics Letters A 171 (3–4) (1992) 199–203.doi:10.1016/0375-9601(92)90426-M
-
[14]
J. S. Richman, J. R. Moorman, Physiological time-series analysis us- ing approximate entropy and sample entropy, American Journal of Physiology—Heart and Circulatory Physiology 278 (6) (2000) H2039– H2049.doi:10.1152/ajpheart.2000.278.6.H2039
-
[15]
S. K. Nayak, A. Bit, A. Dey, B. Mohapatra, K. Pal, A review on the non- linear dynamical system analysis of electrocardiogram signal, Journal of Healthcare Engineering 2018 (2018) 1–19.doi:10.1155/2018/6920420. 52
-
[16]
A. Rosiek, K. Leksowski, The risk factors and prevention of cardiovas- cular disease: the importance of electrocardiogram in the diagnosis and treatment of acute coronary syndrome, Therapeutics and Clinical Risk Management Volume 12 (2016) 1223–1229.doi:10.2147/tcrm.s1078 49
-
[17]
M.Bansal, B.Gandhi, Thegenreofapplicationsrequiringlong-termand continuous monitoring of ecg signals, in: 2017 International Conference on Innovations in Information, Embedded and Communication Systems (ICIIECS), Coimbatore, India, 2017, pp. 1–6.doi:10.1109/ICIIECS. 2017.8275919
-
[18]
M. Bondarenko, C. Menon, M. Elgendi, The role of face regions in re- mote photoplethysmography for contactless heart rate monitoring, npj Digital Medicine 8 (07 2025).doi:10.1038/s41746-025-01814-9. URL https://pmc.ncbi.nlm.nih.gov/articles/PMC12297079/?fbclid= IwY2xjawMrg6hleHRuA2FlbQIxMABicmlkETE4VEdTb3F6Q1Z5R3 FkUk14AR5i_WJOyqBV3O8V7gCIiBL81Yw5lLeXJJsi...
-
[19]
M. G. Bulut, S. Unal, M. Hammad, P. Pławiak, Deep cnn-based detec- tion of cardiac rhythm disorders using ppg signals from wearable devices, PLOSONE20(2025)e0314154.doi:10.1371/journal.pone.0314154. URL https://pmc.ncbi.nlm.nih.gov/articles/PMC11819536/
-
[20]
L.-R. Liu, M.-Y. Huang, S.-T. Huang, L.-C. Kung, C.-h. Lee, W.-T. Yao, M.-F. Tsai, C.-H. Hsu, Y.-C. Chu, F.-H. Hung, H.-W. Chiu, An arrhythmia classification approach via deep learning using single-lead 53 ecg without qrs wave detection, Heliyon 10 (2024) e27200–e27200.doi: 10.1016/j.heliyon.2024.e27200
-
[21]
P. Madan, V. Singh, D. P. Singh, M. Diwakar, B. Pant, A. Kishor, A hybrid deep learning approach for ecg-based arrhythmia classification, Bioengineering 9 (2022) 152.doi:10.3390/bioengineering9040152
-
[22]
A. Panwar, M. Narendra, A. Arya, R. Raj, A. Kumar, Integrated portable ecg monitoring system with cnn classification for early ar- rhythmia detection, Frontiers in Digital Health 7 (03 2025).doi: 10.3389/fdgth.2025.1535335
- [23]
-
[24]
R. Österlund, H. Rekstad, Machine learning models for classification of myocardial infarction using the ptb-xl dataset (2025). URL https://lup.lub.lu.se/student-papers/search/publication/9205011
-
[25]
K. T. Tran, T. N. Tran, D. N. Huynh, N. K. Le, C. D. Le, H. X. Mai, Q. L. Huynh, T. H. Nguyen, A multimodal system for comprehensive cardiovascular monitoring using ecg, pcg, and ppg signal fusion, Sensors 25 (2025) 6708.doi:10.3390/s25216708
-
[26]
A. Minhas, S. C. Pal, K. Jain, Machine learning analysis of integrated abp and ppg signals towards early detection of coronary artery disease, Scientific Reports 15 (03 2025).doi:10.1038/s41598-025-93390-x. URL https://www.nature.com/articles/s41598-025-93390-x 54
-
[27]
T. Oladunni, A. Wong, Rethinking multimodality: Optimizing multi- modal deep learning for biomedical signal classification, IEEE Access 13 (2025) 156436–156464.doi:10.1109/ACCESS.2025.3605315
-
[28]
L. Niu, C. Chen, H. Liu, S. Zhou, M. Shu, A deep-learning approach to ecg classification based on adversarial domain adaptation, Healthcare 8 (2020) 437.doi:10.3390/healthcare8040437
-
[29]
S.Liu, N.Wang, Z.Wang, N.Zeng, R.Pachori, D.Wang, Self-supervised learning of ecg and ppg signals for multi-modal health monitoring, Pro- ceedings of Machine Learning Research 278 (2025) 1–9
work page 2025
-
[30]
A. Anand, A. Dargar, Comparative analysis of the diagnostic potential ofunimodalandmultimodalphysiologicalsignalsforstressclassification, Journal of Pediatric Neurosciences (03 2026).doi:10.4103/jpn.jpn_ 154_25. URL https://journals.lww.com/jopn/fulltext/9900/comparative_anal ysis_of_the_diagnostic_potential.127.aspx
-
[31]
C. Ding, C. Wu, Self-supervised learning for biomedical signal process- ing: A systematic review on ecg and ppg signals (2024)
work page 2024
-
[32]
Takens, Detecting strange attractors in turbulence, in: Dynamical Systems and Turbulence, Vol
F. Takens, Detecting strange attractors in turbulence, in: Dynamical Systems and Turbulence, Vol. 898 of Lecture Notes in Mathematics, Springer, 1981, pp. 366–381.doi:10.1007/BFb0091924
-
[33]
A. M. Fraser, H. L. Swinney, Independent coordinates for strange attrac- tors from mutual information, Physical Review A 33 (2) (1986) 1134– 1140.doi:10.1103/PhysRevA.33.1134. 55
-
[34]
M. T. Rosenstein, J. J. Collins, C. J. De Luca, A practical method for calculating largest Lyapunov exponents from small data sets, Physica D: Nonlinear Phenomena 65 (1–2) (1993) 117–134.doi:10.1016/0167 -2789(93)90009-P
-
[35]
The LUMIERE dataset: Longitudinal Glioblastoma MRI with expert RANO evaluation
P. Wagner, N. Strodthoff, R.-D. Bousseljot, D. Kreiseler, F. I. Lunze, W. Samek, T. Schaeffter, PTB-XL, a large publicly available electrocar- diography dataset, Scientific Data 7 (2020) 154.doi:10.1038/s41597 -020-0495-6
-
[36]
A. Nemcova, E. Vargova, R. Smisek, L. Marsanova, L. Smital, M. Vitek, Brno university of technology smartphone PPG database (BUT PPG): Annotated dataset for PPG quality assessment and heart rate esti- mation, BioMed Research International 2021 (2021) 3453007.doi: 10.1155/2021/3453007
-
[37]
B. Moody, G. Moody, M. Villarroel, G. D. Clifford, I. Silva, MIMIC-III waveform database, PhysioNet (2016).doi:10.13026/C2607M
-
[38]
S. Jokic, et al., Large-scale real-world smartphone photoplethysmog- raphy datasets for vascular assessment, Electronics 15 (5) (2026) 988. doi:10.3390/electronics15050988
-
[39]
T. G. Dietterich, Ensemble methods in machine learning, in: Multiple Classifier Systems, Springer, Berlin, Heidelberg, 2000, pp. 1–15.doi: 10.1007/3-540-45014-9_1
-
[40]
K. Bertsch, D. Hagemann, E. Naumann, H. Schachinger, Stability of heart rate variability indices reflecting parasympathetic activity, Psy- 56 chophysiology 49 (5) (2012) 672–682.doi:10.1111/j.1469-8986.20 11.01341.x
- [41]
-
[42]
M. B. Kennel, R. Brown, H. D. I. Abarbanel, Determining embedding dimension for phase-space reconstruction using a geometrical construc- tion, Physical Review A 45 (6) (1992) 3403–3411.doi:10.1103/Phys RevA.45.3403
-
[43]
X. Ding, B. P. Yan, Y.-T. Zhang, J. Liu, N. Zhao, H. K. Tsang, Pulse transit time based continuous cuffless blood pressure estimation: A new extension and a comprehensive evaluation, Scientific Reports 7 (1) (2017) 11554.doi:10.1038/s41598-017-11507-3
-
[44]
Z.-B. Zhou, T.-R. Cui, D. Li, J.-M. Jian, Z. Li, S.-R. Ji, X. Li, J.-D. Xu, H.-F. Liu, Y. Yang, T.-L. Ren, Wearable continuous blood pressure monitoring devices based on pulse wave transit time and pulse arrival time: A review, Materials 16 (6) (2023) 2133.doi:10.3390/ma160621 33. 57
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.