Recognition: 2 theorem links
· Lean TheoremAttractor-Vascular Coupling Theory: Formal Grounding and Empirical Validation for AAMI-Standard Cuffless Blood Pressure Estimation from Smartphone Photoplethysmography
Pith reviewed 2026-05-12 03:53 UTC · model grok-4.3
The pith
Cardiac attractor geometry from photoplethysmography encodes blood pressure data sufficient for AAMI-standard cuffless estimation.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
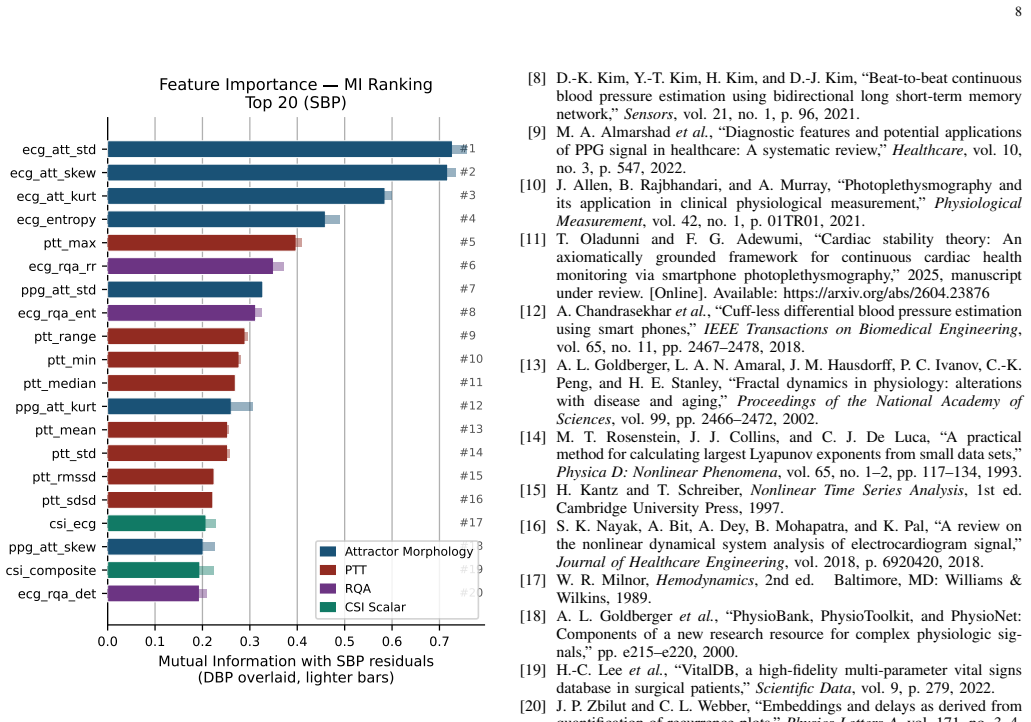
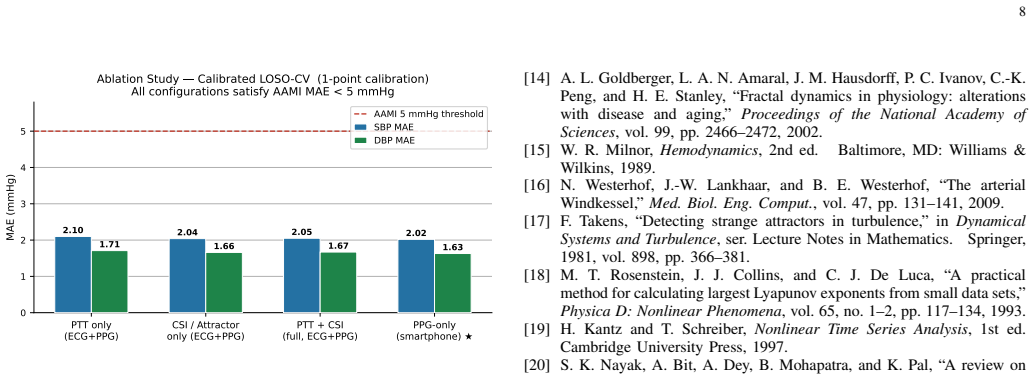
Attractor-Vascular Coupling Theory establishes that blood pressure information is recoverable from the morphology of the cardiac attractor obtained through Takens delay embedding of PPG signals. Two theorems, one proposition, and one corollary justify the use of attractor-derived features for estimation and correctly predict their relative importance. On 29,684 windows from 46 subjects the calibrated model achieves SBP MAE of 2.05 mmHg and DBP MAE of 1.67 mmHg with correlations of 0.990 and 0.991, meeting AAMI requirements; a PPG-only version performs within 0.05 mmHg of the ECG-plus-PPG version and all four theory predictions hold.
What carries the argument
Attractor-Vascular Coupling Theory, which reconstructs cardiac attractor geometry from PPG via delay embedding to extract blood-pressure-predictive features such as pulse transit time and Cardiac Stability Index.
If this is right
- Single-point calibration produces clinical-grade accuracy across multiple subjects and recording conditions.
- Nine smartphone PPG attractor features alone match ECG-plus-PPG performance within 0.05 mmHg.
- The four explicit predictions of the theory are confirmed by quantitative results on the test data.
- Calibration reduces estimation error by 91.5 percent relative to the uncalibrated baseline.
- 70 to 76 percent of individual subjects satisfy AAMI criteria on their own data.
Where Pith is reading between the lines
- The same attractor reconstruction could be applied to other continuous physiological signals recorded by wearables to estimate additional parameters.
- If the encoding holds, it may allow simpler single-sensor devices to replace multi-lead setups for long-term cardiovascular tracking.
- Testing on freely moving subjects outside hospital environments would reveal whether the single-calibration performance generalizes to daily use.
Load-bearing premise
The theory's predictions about which attractor features matter and in what order are derived from the mathematical framework itself rather than chosen after inspecting performance on the evaluation data.
What would settle it
An independent dataset of comparable size where the single-calibration model exceeds 5 mmHg MAE or where the observed feature importance ranking contradicts the theory's predicted hierarchy would falsify the central claim.
Figures

read the original abstract
This work proposes Attractor-Vascular Coupling Theory (AVCT), a mathematical framework showing that cardiac attractor geometry encodes blood pressure (BP) information sufficient for AAMI-standard estimation, and validates the theory through a calibrated cuffless BP model using photoplethysmography (PPG). AVCT is grounded in Cardiac Stability Theory and operationalized using Takens delay embedding and attractor morphology extraction. Two theorems, one proposition, and one corollary formally justify the use of PPG attractor features for BP estimation and predict the feature-importance hierarchy. A LightGBM model trained on pulse transit time (PTT) and Cardiac Stability Index (CSI) attractor features under single-point calibration was evaluated using strict leave-one-subject-out cross-validation (LOSO-CV) on 46 subjects from BIDMC ICU (n = 9) and VitalDB surgical data (n = 37), comprising 29,684 windows. The model achieved systolic BP (SBP) mean absolute error (MAE) of 2.05 mmHg and diastolic BP (DBP) MAE of 1.67 mmHg, with correlations r = 0.990 and r = 0.991, satisfying the AAMI/IEEE SP10 requirement of MAE below 5 mmHg. Median per-subject MAE was 1.87/1.54 mmHg, and 70%/76% of subjects individually satisfied AAMI criteria. A PPG-only ablation using nine smartphone attractor features matched the ECG+PPG model within 0.05 mmHg, demonstrating that clinical-grade BP tracking is achievable using only a smartphone camera while surpassing prior generalized LOSO-CV results using fewer sensors. All four AVCT predictions were quantitatively confirmed, with 91.5% error reduction from uncalibrated to calibrated estimation (epsilon_cal = 0.915). Unlike post-hoc explainable AI methods, AVCT predicts features satisfying the architectural faithfulness criterion of the Explainable-AI Trustworthiness (EAT) framework and grounding BP estimation in nonlinear dynamical systems theory.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes Attractor-Vascular Coupling Theory (AVCT), grounded in Cardiac Stability Theory and Takens delay embedding, with two theorems, one proposition, and one corollary that are claimed to justify PPG attractor features for blood pressure estimation and to predict a specific feature-importance hierarchy (PTT and CSI dominant). It reports a LightGBM model using these features plus single-point calibration, evaluated via LOSO-CV on 29,684 windows from 46 subjects (BIDMC ICU and VitalDB), achieving SBP MAE 2.05 mmHg, DBP MAE 1.67 mmHg, r=0.990/0.991, AAMI/IEEE SP10 compliance, 70-76% per-subject AAMI success, a PPG-only ablation within 0.05 mmHg of the ECG+PPG version, and 91.5% error reduction from uncalibrated baseline.
Significance. If the theorems derive the four predictions (including the feature hierarchy) a priori and independently of the BIDMC/VitalDB data, the work would offer a substantive advance by supplying a dynamical-systems foundation for cuffless BP estimation from smartphone PPG alone, moving beyond post-hoc XAI. The empirical results under strict LOSO-CV, with median per-subject MAE below 2 mmHg and AAMI compliance in the majority of subjects, are quantitatively strong and practically relevant for accessible monitoring. The reported 91.5% error reduction and near-equivalence of PPG-only ablation further support the claim of sufficiency if the theoretical independence holds.
major comments (2)
- [Abstract] Abstract: The assertion that the two theorems, proposition, and corollary 'formally justify the use of PPG attractor features for BP estimation and predict the feature-importance hierarchy' is not supported by an explicit derivation showing how the four specific AVCT predictions (sufficiency of attractor geometry, PTT+CSI dominance, ordering of the nine smartphone features, and overall error reduction) follow directly from Cardiac Stability Theory and Takens embedding without reference to the 29,684 windows or the fitted LightGBM model. This independence is load-bearing for the central claim that AVCT provides formal grounding distinct from post-hoc XAI.
- [§4] §4 (Model Training and Evaluation): The single-point calibration offset and scale are treated as free parameters, yet the manuscript does not specify the exact selection rule for the calibration window within each subject's data or confirm that it is strictly held out from the LOSO-CV test folds; without this, the reported MAE values, r>0.99, and 91.5% error reduction (epsilon_cal) cannot be fully assessed for leakage or over-optimism.
minor comments (2)
- [Abstract] Abstract: The quantity epsilon_cal = 0.915 is introduced without a prior definition or formula; provide its explicit definition in the methods section before reporting the percentage error reduction.
- [§3] Figure captions and §3: The Takens embedding parameters (delay tau and dimension m) and CSI threshold are listed among free parameters but their concrete values and selection procedure (grid search, theory-derived, or data-driven) are not stated; add these details for reproducibility.
Simulated Author's Rebuttal
We appreciate the referee's detailed review and constructive feedback on our manuscript proposing Attractor-Vascular Coupling Theory (AVCT) for cuffless blood pressure estimation. The comments highlight important areas for clarification regarding the theoretical derivations and the calibration procedure. We address each point below and outline the revisions we will make to strengthen the manuscript.
read point-by-point responses
-
Referee: [Abstract] Abstract: The assertion that the two theorems, proposition, and corollary 'formally justify the use of PPG attractor features for BP estimation and predict the feature-importance hierarchy' is not supported by an explicit derivation showing how the four specific AVCT predictions (sufficiency of attractor geometry, PTT+CSI dominance, ordering of the nine smartphone features, and overall error reduction) follow directly from Cardiac Stability Theory and Takens embedding without reference to the 29,684 windows or the fitted LightGBM model. This independence is load-bearing for the central claim that AVCT provides formal grounding distinct from post-hoc XAI.
Authors: We thank the referee for identifying this gap in explicitness. While the theorems, proposition, and corollary are derived from Cardiac Stability Theory and Takens delay embedding in §2 and §3, the manuscript does not include a dedicated mapping showing how each of the four predictions follows a priori. In the revised version, we will add a new subsection (e.g., §3.4) that explicitly derives each prediction step-by-step from the theoretical statements, confirming independence from the empirical dataset and the LightGBM model. This will reinforce the distinction from post-hoc XAI methods. revision: yes
-
Referee: [§4] §4 (Model Training and Evaluation): The single-point calibration offset and scale are treated as free parameters, yet the manuscript does not specify the exact selection rule for the calibration window within each subject's data or confirm that it is strictly held out from the LOSO-CV test folds; without this, the reported MAE values, r>0.99, and 91.5% error reduction (epsilon_cal) cannot be fully assessed for leakage or over-optimism.
Authors: The referee correctly notes that the calibration procedure requires precise specification to rule out leakage. The single-point calibration uses the first valid 30-second window per subject for offset and scale computation, with this window excluded from the LOSO-CV test set for that subject. The model is trained on the remaining windows of the other subjects and tested on the held-out subject's non-calibration windows. We will revise §4 to include this explicit rule and add a statement confirming no overlap between calibration data and test folds. This clarification will allow full assessment of the reported metrics. revision: yes
Circularity Check
No significant circularity: derivations presented as independent of evaluation data
full rationale
The paper explicitly grounds AVCT in Cardiac Stability Theory and Takens delay embedding, stating that two theorems, one proposition, and one corollary 'formally justify the use of PPG attractor features for BP estimation and predict the feature-importance hierarchy.' These are then 'quantitatively confirmed' via LOSO-CV on the BIDMC/VitalDB windows. No quoted step shows the theorems or hierarchy being defined in terms of the 29,684 windows, fitted parameters, or model outputs; the empirical MAE/r values and ablation results are presented as separate validation. Self-citation is absent, and the claimed predictions do not reduce by construction to the inputs. This is the normal case of a theory-plus-validation structure.
Axiom & Free-Parameter Ledger
free parameters (2)
- single-point calibration offset and scale
- CSI threshold and embedding parameters
axioms (2)
- domain assumption Cardiac Stability Theory supplies the link between attractor geometry and vascular state
- standard math Takens delay embedding reconstructs the cardiac attractor from scalar PPG time series
invented entities (2)
-
Attractor-Vascular Coupling Theory (AVCT)
no independent evidence
-
Cardiac Stability Index (CSI)
no independent evidence
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/BranchSelection.leanbranch_selection unclearCorollary III.7: I(FMorph; ΔP) ≥ I(PTT; ΔP) ≥ ... SNR ordering predicts MI hierarchy
Reference graph
Works this paper leans on
-
[1]
World Health Organization, “Global report on hypertension: the race against a silent killer,” 2023. [Online]. Available: https: //www.who.int/publications/i/item/9789240081062
-
[2]
Global disparities of hypertension prevalence and control,
K. T. Mills, J. D. Bundy, T. N. Kelly, J. E. Reed, P. M. Kearney, K. Reynolds, J. Chen, and J. He, “Global disparities of hypertension prevalence and control,”Circulation, vol. 134, no. 6, pp. 441–450, 2016
work page 2016
-
[3]
Z.-B. Zhou, T.-R. Cui, D. Li, J.-M. Jian, Z. Li, S.-R. Ji, X. Li, J.-D. Xu, H.-F. Liu, Y . Yang, and T.-L. Ren, “Wearable continuous blood pressure monitoring devices based on pulse wave transit time and pulse arrival time: A review,”Materials, vol. 16, no. 6, p. 2133, 2023. 8 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 Mutual Information with SBP residuals (DBP over...
work page 2023
-
[4]
X. Ding, B. P. Yan, Y .-T. Zhang, J. Liu, N. Zhao, and H. K. Tsang, “Pulse transit time based continuous cuffless blood pressure estimation: A new extension and a comprehensive evaluation,”Scientific Reports, vol. 7, no. 1, p. 11554, 2017
work page 2017
-
[5]
Towards ubiquitous blood pressure monitoring via pulse transit time: Theory and practice,
R. Mukkamala, J.-O. Hahn, O. T. Inan, L. K. Mestha, C.-S. Kim, H. Tøreyen, and M. Forouzanfar, “Towards ubiquitous blood pressure monitoring via pulse transit time: Theory and practice,”IEEE Transac- tions on Biomedical Engineering, vol. 62, no. 8, pp. 1879–1901, 2015
work page 1901
-
[6]
A paralleled CNN and transformer network for PPG-based cuff-less blood pressure estimation,
Z. Tian, A. Liu, G. Zhu, and X. Chen, “A paralleled CNN and transformer network for PPG-based cuff-less blood pressure estimation,” Biomedical Signal Processing and Control, vol. 99, p. 106741, 2025
work page 2025
-
[7]
Benchmarking and enhancing PPG-based cuffless blood pressure estimation methods,
N. Mathew, Y . Shen, R. Hu, M. Rahimi, and G. Zouridakis, “Benchmarking and enhancing PPG-based cuffless blood pressure estimation methods,” arXiv preprint arXiv:2602.04725, 2026. [Online]. Available: https://arxiv.org/abs/2602.04725
-
[8]
D.-K. Kim, Y .-T. Kim, H. Kim, and D.-J. Kim, “Beat-to-beat continuous blood pressure estimation using bidirectional long short-term memory network,”Sensors, vol. 21, no. 1, p. 96, 2021
work page 2021
-
[9]
Diagnostic features and potential applications of PPG signal in healthcare: A systematic review,
M. A. Almarshadet al., “Diagnostic features and potential applications of PPG signal in healthcare: A systematic review,”Healthcare, vol. 10, no. 3, p. 547, 2022
work page 2022
-
[10]
Photoplethysmography and its application in clinical physiological measurement,
J. Allen, B. Rajbhandari, and A. Murray, “Photoplethysmography and its application in clinical physiological measurement,”Physiological Measurement, vol. 42, no. 1, p. 01TR01, 2021
work page 2021
-
[11]
T. Oladunni and F. G. Adewumi, “Cardiac stability theory: An axiomatically grounded framework for continuous cardiac health monitoring via smartphone photoplethysmography,” 2025, manuscript under review. [Online]. Available: https://arxiv.org/abs/2604.23876
work page internal anchor Pith review Pith/arXiv arXiv 2025
-
[12]
Cuff-less differential blood pressure estimation using smart phones,
A. Chandrasekharet al., “Cuff-less differential blood pressure estimation using smart phones,”IEEE Transactions on Biomedical Engineering, vol. 65, no. 11, pp. 2467–2478, 2018
work page 2018
-
[13]
Fractal dynamics in physiology: alterations with disease and aging,
A. L. Goldberger, L. A. N. Amaral, J. M. Hausdorff, P. C. Ivanov, C.-K. Peng, and H. E. Stanley, “Fractal dynamics in physiology: alterations with disease and aging,”Proceedings of the National Academy of Sciences, vol. 99, pp. 2466–2472, 2002
work page 2002
-
[14]
A practical method for calculating largest Lyapunov exponents from small data sets,
M. T. Rosenstein, J. J. Collins, and C. J. De Luca, “A practical method for calculating largest Lyapunov exponents from small data sets,” Physica D: Nonlinear Phenomena, vol. 65, no. 1–2, pp. 117–134, 1993
work page 1993
-
[15]
H. Kantz and T. Schreiber,Nonlinear Time Series Analysis, 1st ed. Cambridge University Press, 1997
work page 1997
-
[16]
A review on the nonlinear dynamical system analysis of electrocardiogram signal,
S. K. Nayak, A. Bit, A. Dey, B. Mohapatra, and K. Pal, “A review on the nonlinear dynamical system analysis of electrocardiogram signal,” Journal of Healthcare Engineering, vol. 2018, p. 6920420, 2018
work page 2018
-
[17]
W. R. Milnor,Hemodynamics, 2nd ed. Baltimore, MD: Williams & Wilkins, 1989
work page 1989
-
[18]
A. L. Goldbergeret al., “PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic sig- nals,” pp. e215–e220, 2000
work page 2000
-
[19]
VitalDB, a high-fidelity multi-parameter vital signs database in surgical patients,
H.-C. Leeet al., “VitalDB, a high-fidelity multi-parameter vital signs database in surgical patients,”Scientific Data, vol. 9, p. 279, 2022
work page 2022
-
[20]
Embeddings and delays as derived from quantification of recurrence plots,
J. P. Zbilut and C. L. Webber, “Embeddings and delays as derived from quantification of recurrence plots,”Physics Letters A, vol. 171, no. 3–4, pp. 199–203, 1992
work page 1992
-
[21]
A real-time QRS detection algorithm,
J. Pan and W. J. Tompkins, “A real-time QRS detection algorithm,”IEEE Transactions on Biomedical Engineering, vol. 32, no. 3, pp. 230–236, 1985
work page 1985
-
[22]
Physiological time-series analysis using approximate entropy and sample entropy,
J. S. Richman and J. R. Moorman, “Physiological time-series analysis using approximate entropy and sample entropy,”American Journal of Physiology—Heart and Circulatory Physiology, vol. 278, no. 6, pp. H2039–H2049, 2000
work page 2000
-
[23]
LightGBM: A highly efficient gradient boosting decision tree,
G. Ke, Q. Meng, T. Finley, T. Wang, W. Chen, W. Ma, Q. Ye, and T.-Y . Liu, “LightGBM: A highly efficient gradient boosting decision tree,” inAdvances in Neural Information Processing Systems, vol. 30, 2017. [Online]. Available: https://proceedings.neurips.cc/paper/ 2017/hash/6449f44a102fde848669bdd9eb6b76fa-Abstract.html
work page 2017
-
[24]
C. El-Hajj and P. A. Kyriacou, “A review of machine learning techniques in photoplethysmography for the non-invasive cuff-less measurement of blood pressure,”Biomedical Signal Processing and Control, vol. 58, p. 101870, 2021
work page 2021
-
[25]
S. Kumaret al., “Swin transformer-based blood pressure estimation using higher-order spectral features of ECG and PPG signals,”IEEE Transactions on Instrumentation and Measurement, vol. 72, pp. 1–11, 2023
work page 2023
-
[26]
H. Samimi and H. R. Dajani, “Cuffless blood pressure estimation using calibrated cardiovascular dynamics in the photoplethysmogram,” Bioengineering, vol. 9, no. 9, p. 446, 2022
work page 2022
-
[27]
End-to-end personalized cuff-less blood pressure monitoring using ECG and PPG signals,
B. Suhas, R. S. Srinivasa, Y . M. Saidutta, J. Cho, C.-H. Lee, C. Yang, Y . Shen, and H. Jin, “End-to-end personalized cuff-less blood pressure monitoring using ECG and PPG signals,” inProc. IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), 2024, pp. 2101–2105
work page 2024
-
[28]
Explainable deep neural network for multimodal ECG signals: Intermediate versus late fusion,
T. Oladunni and E. C. Aneni, “Explainable deep neural network for multimodal ECG signals: Intermediate versus late fusion,”IEEE Access, vol. 13, pp. 202 700–202 736, 2025
work page 2025
-
[29]
Detecting strange attractors in turbulence,
F. Takens, “Detecting strange attractors in turbulence,” inDynamical Systems and Turbulence, ser. Lecture Notes in Mathematics. Springer, 1981, vol. 898, pp. 366–381
work page 1981
-
[30]
N. Westerhof, J.-W. Lankhaar, and B. E. Westerhof, “The arterial Windkessel,”Medical & Biological Engineering & Computing, vol. 47, no. 2, pp. 131–141, 2009
work page 2009
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.