Recognition: unknown
Effect of the dose distribution and organ architecture on the toxicity in FLASH radiotherapy: a modeling study
Pith reviewed 2026-05-07 14:00 UTC · model grok-4.3
The pith
If the FLASH effect works locally, it spares toxicity more in serial organs than in parallel organs.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
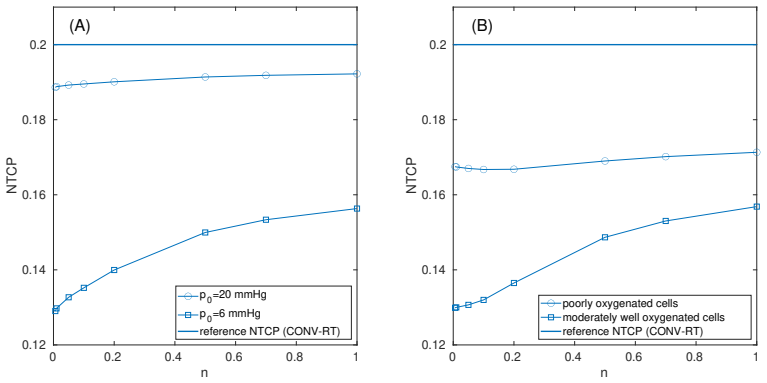
Both the radiolytic oxygen depletion model and a logistic phenomenological model predict FLASH-induced toxicity sparing that increases as the organ architecture shifts from parallel (volume effect parameter n=1) to serial (n approaching 0). For instance, with conventional NTCP set to 0.2, FLASH NTCP drops to 0.14 for n=1 but to 0.11 for n=0.1 under the same inhomogeneous dose distribution.
What carries the argument
Combination of local FLASH dose modification models (ROD or logistic function of dose and rate) with the Lyman-Kutcher-Burman NTCP model, where the volume effect parameter n controls sensitivity to dose distribution inhomogeneity.
If this is right
- FLASH radiotherapy lowers the predicted normal tissue complication probability relative to conventional delivery.
- The magnitude of this lowering grows larger for smaller values of the volume parameter n, corresponding to serial organ architecture.
- Serial organs benefit more because they are more sensitive to localized high doses, which the local FLASH models reduce preferentially.
- Organ architecture must be accounted for when estimating the clinical advantage of FLASH delivery.
Where Pith is reading between the lines
- Clinical studies might observe stronger FLASH benefits in treatments targeting serial structures such as the spinal cord.
- Radiotherapy planning systems could incorporate organ-specific architecture when optimizing FLASH plans to maximize sparing.
- Further modeling could test how non-local mechanisms would alter the dependence on architecture.
Load-bearing premise
The protective FLASH effect arises from mechanisms that depend solely on the local dose and local dose rate within small regions of the tissue.
What would settle it
Direct measurement of complication rates in serial versus parallel organs irradiated with identical inhomogeneous dose distributions using FLASH versus conventional delivery.
Figures


read the original abstract
Objective: This study aims to investigate the influence of organ architecture (specifically the distinction between serial and parallel tissue) on the protective FLASH effect when organs are irradiated with inhomogeneous dose distributions. Approach: An in silico modeling framework was developed using two distinct methods to calculate the effective FLASH dose: the first method utilized a biophysical model of radiolytic oxygen depletion (ROD); the second employed a phenomenological logistic function where the effective FLASH dose is a function of local dose and dose rate. Both models assume that the underlying mechanism behind the FLASH effect is local. Normal Tissue Complication Probability (NTCP) for heterogeneous dose distributions was calculated using the Lyman-Kutcher-Burman (LKB) model and the generalized equivalent uniform dose, varying the volume effect parameter n from 1.0 (parallel) to below 0.01 (serial) to explore different architectures. Results: Both the ROD and phenomenological models showed FLASH sparing compared to conventional radiotherapy. Also, the sparing increased with decreasing $n$ (the sparing is more important for serial organs). For example, for a specific calculation, when the NTCP for conventional radiotherapy was 0.2 (set value) the corresponding NTCP for FLASH delivery ranged from 0.14 for n=1 to 0.11 for n=0.1. Significance: Our results indicate that if the underlying mechanism/s behind the FLASH effect is/are local, the toxicity sparing associated to FLASH-RT can be dependent on the architecture of the irradiated organ/tissue, being more important for serial organs, which are more sensitive to large local doses than to average doses.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript develops an in silico modeling framework to examine the dependence of FLASH radiotherapy toxicity sparing on organ architecture for inhomogeneous dose distributions. Two local-mechanism models (radiolytic oxygen depletion and a phenomenological logistic function) are used to derive effective FLASH dose maps from local dose and dose-rate information; these maps are then fed into the standard Lyman-Kutcher-Burman NTCP calculation via generalized EUD while parametrically varying the volume-effect parameter n from 1.0 (parallel) to <0.01 (serial). The central result is that NTCP reduction is larger at low n, implying greater sparing for serial organs under the local-mechanism premise.
Significance. If the local-mechanism premise holds, the architecture dependence identified here is clinically relevant because serial organs are known to be limited by hot-spot doses rather than mean dose; the parametric exploration of n therefore supplies a clear, falsifiable prediction for which tissues should show the strongest FLASH benefit. Credit is due for the consistent, non-circular application of two independent prior FLASH models, the standard LKB/EUD formalism, and the explicit conditioning of all claims on the locality assumption.
major comments (1)
- The main limitation noted is the absence of any direct comparison between the modeled NTCP reductions and existing experimental or clinical FLASH data; while the modeling itself is internally consistent, adding even a qualitative discussion of how the predicted n-dependence could be tested against published rodent or patient outcomes would strengthen the bridge from simulation to experiment.
minor comments (2)
- The example NTCP values (conventional 0.2, FLASH 0.14 at n=1 and 0.11 at n=0.1) are useful but would be easier to interpret if the underlying dose distribution, organ volume, and specific parameter values for the ROD or logistic model were stated explicitly in the results or methods.
- A brief sentence recalling the definition of the generalized EUD and the role of n in the LKB model would help readers outside the NTCP community follow the monotonicity argument without consulting external references.
Simulated Author's Rebuttal
We thank the referee for the positive evaluation and the recommendation for minor revision. The suggestion to strengthen the connection to experiment is appreciated, and we will incorporate a qualitative discussion as proposed.
read point-by-point responses
-
Referee: The main limitation noted is the absence of any direct comparison between the modeled NTCP reductions and existing experimental or clinical FLASH data; while the modeling itself is internally consistent, adding even a qualitative discussion of how the predicted n-dependence could be tested against published rodent or patient outcomes would strengthen the bridge from simulation to experiment.
Authors: We agree that the manuscript, being an in silico modeling study, does not contain direct comparisons to experimental or clinical FLASH data. This is a genuine scope limitation rather than an oversight. To address the referee's point, we will add a qualitative discussion (likely in a new subsection of the Discussion) outlining how the predicted stronger NTCP reduction at low n (serial architecture) under local mechanisms could be tested. Examples include referencing existing rodent FLASH studies on serial organs such as the spinal cord or esophagus versus parallel organs such as lung, or suggesting designs for future experiments that isolate hot-spot versus mean-dose effects. This addition will provide falsifiable predictions without claiming empirical validation in the current work. revision: yes
Circularity Check
No significant circularity
full rationale
The paper's chain applies two external models (ROD biophysical and logistic phenomenological) pointwise to local dose-rate maps under an explicitly stated local-mechanism assumption, then feeds the resulting effective-dose distribution into the standard LKB NTCP model with generalized EUD while parametrically varying the volume parameter n. The reported trend (greater NTCP reduction at low n) is a direct mathematical consequence of the EUD definition for serial-like organs and does not reduce any reported quantity to a fit or definition taken from the same data. No self-citation is load-bearing; all core components are drawn from prior independent literature or standard radiobiological formalism. The central claim remains conditional on the local-mechanism premise and contains independent content.
Axiom & Free-Parameter Ledger
free parameters (2)
- volume effect parameter n
- logistic function parameters
axioms (2)
- domain assumption The FLASH effect is produced by local processes only (radiolytic oxygen depletion or local dose-rate response).
- standard math The Lyman-Kutcher-Burman model with generalized EUD accurately captures normal-tissue complication probability for heterogeneous doses.
Reference graph
Works this paper leans on
-
[1]
Favaudon, L
V. Favaudon, L. Caplier, V. Monceau, F. Pouzoulet, M. Sayarat h, C. Fouillade, et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Sci. Transl. Med., 6(245):245ra93, 2014
2014
-
[2]
Montay-Gruel, K
P. Montay-Gruel, K. Petersson, M. Jaccard, G. Boivin, J. F. Ge rmond, B. Petit, et al. Irradiation in a flash: Unique sparing of memory in mice after whole brain irradiation with dose rates above 100 Gy/s. Radiother. Oncol., 124(3):365–369, 2017
2017
-
[3]
Montay-Gruel, A
P. Montay-Gruel, A. Bouchet, M. Jaccard, D. Patin, R. Serduc , W. Aim, et al. X-rays can trigger the FLASH effect: Ultra-high dose-rate s yn- chrotron light source prevents normal brain injury after whole br ain irradiation in mice. Radiother. Oncol., 129(3):582–588, 2018
2018
-
[4]
M. C. Vozenin, P. De Fornel, K. Petersson, V. Favaudon, M. Jac card, J. F. Germond, et al. The advantage of FLASH radiotherapy confir med xiii in mini-pig and cat-cancer patients. Clin. Cancer Res. , 25(1):35–42, 2019
2019
-
[5]
Montay-Gruel, M
P. Montay-Gruel, M. M. Acharya, K. Petersson, L. Alikhani, C. Y akkala, B. D. Allen, et al. Long-term neurocognitive benefits of FLASH radiotherapy driven by reduced reactive oxygen species. PNAS, 116(22):10943–10951, 2019
2019
-
[6]
K. Levy, S. Natarajan, J. Wang, S. Chow, J. T. Eggold, P. E. Lo o, et al. Abdominal FLASH irradiation reduces radiation-induced gastrointe sti- nal toxicity for the treatment of ovarian cancer in mice. Sci. Rep. , 10(1):21600, 2020
2020
-
[7]
E. S. Diffenderfer, I. I. Verginadis, M. M. Kim, K. Shoniyozov, A. Ve- lalopoulou, D. Goia, et al. Design, implementation, and in vivo valida- tion of a novel proton FLASH radiation therapy system. Int. J. Radiat. Oncol. Biol. Phys. , 106(2):440–448, 2020
2020
-
[8]
Liljedahl, E
E. Liljedahl, E. Konradsson, E. Gustafsson, K. F¨ ornvik Jonss on, J. K. Olofsson, C. Ceberg, et al. Long-term anti-tumor effects following both conventional radiotherapy and FLASH in fully immunocompetent ani- mals with glioblastoma. Sci. Rep. , 12(1):1–12, 2022
2022
-
[9]
F. Gao, Y. Yang, H. Zhu, J. Wang, D. Xiao, Z. Zhou, et al. First demonstration of the FLASH effect with ultrahigh dose rate high-en ergy X-rays. Radiother. Oncol., 166:44–50, 2022
2022
-
[10]
Favaudon, R
V. Favaudon, R. Labarbe, and C. L. Limoli. Model studies of the role of oxygen in the FLASH effect. Med. Phys. , 49(3):2068–2081, 2022
2068
-
[11]
Pratx and D
G. Pratx and D. S. Kapp. A computational model of radiolytic ox y- gen depletion during FLASH irradiation and its effect on the oxygen enhancement ratio. Phys. Med. Biol. , 64(18):185005, 2019
2019
-
[12]
Pratx and D
G. Pratx and D. S. Kapp. Ultra-high-dose-rate FLASH irradiat ion may spare hypoxic stem cell niches in normal tissues. Int. J. Radiat. Oncol. Biol. Phys. , 105(1):190–192, 2019
2019
-
[13]
Petersson, G
K. Petersson, G. Adrian, K. Butterworth, and S. J. McMahon . A quanti- tative analysis of the role of oxygen tension in FLASH radiation thera py. Int. J. Radiat. Oncol. Biol. Phys. , 107(3):539–547, 2020. xiv
2020
-
[14]
X. Cao, R. Zhang, T. V. Esipova, S. R. Allu, R. Ashraf, M. Rahma n, et al. Quantification of oxygen depletion during FLASH irradiation in vitro and in vivo. Int. J. Radiat. Oncol. Biol. Phys. , 111(1):240–248, 2021
2021
-
[15]
El Khatib, A
M. El Khatib, A. L. Van Slyke, A. Velalopoulou, M. M. Kim, K. Shoniy - ozov, S. R. Allu, et al. Ultrafast tracking of oxygen dynamics during proton FLASH. Int. J. Radiat. Oncol. Biol. Phys. , 113(3):624–634, 2022
2022
-
[16]
B. Ha, K. Liang, C. Liu, S. Melemenidis, R. Manjappa, V. Viswanat han, et al. Real-time optical oximetry during FLASH radiotherapy using a phosphorescent nanoprobe. Radiother. Oncol., 176:239–243, 2022
2022
-
[17]
Boscolo, E
D. Boscolo, E. Scifoni, M. Durante, M. Kr¨ amer, and M. C. Fuss . May oxygen depletion explain the FLASH effect? A chemical track struct ure analysis. Radiother. Oncol., 162:68–75, 2021
2021
-
[18]
Jansen, E
J. Jansen, E. Beyreuther, D. Garc ´ ıa-Calder´ on, L. Karsch , J. Knoll, J. Pawelke, et al. Changes in radical levels as a cause for the FLASH e f- fect: Impact of beam structure parameters at ultra-high rates on oxygen depletion in water. Radiother. Oncol., 175:193–196, 2022
2022
-
[19]
C. L. Limoli and M-C. Vozenin. Reinventing radiobiology in the light o f flash radiotherapy. Annual Review of Cancer Biology , 7(1):1–21, 2023
2023
-
[20]
D. R. Spitz, G. R. Buettner, M. S. Petronek, J. J. St-Aubin, R . T. Flynn, T. J. Waldron, et al. An integrated physico-chemical approach for ex- plaining the differential impact of FLASH versus conventional dose r ate irradiation on cancer and normal tissue responses. Radiother. Oncol. , 139:23–27, 2019
2019
-
[21]
J. Y. Jin, A. Gu, W. Wang, N. L. Oleinick, M. Machtay, and K. Feng - Ming. Ultra-high dose rate effect on circulating immune cells: A po- tential mechanism for FLASH effect? Radiother. Oncol. , 149:55–62, 2020
2020
-
[22]
Abolfath, A
R. Abolfath, A. Baikalov, A. Fraile, S. Bartzsch, E. Sch¨ uler, a nd R. Mo- han. A stochastic reaction–diffusion modeling investigation of FLASH ultra-high dose rate response in different tissues. Frontiers in Physics , 11:1060910, 2023. xv
2023
-
[23]
H. Ni, Z. J. Reitman, W. Zou, M. N. Akhtar, R. Paul, M. Huang, D. Zhang, H. Zheng, R. Zhang, R. Ma, G. Ngo, L. Zhang, E. S. Diff- enderfer, S. A. O. Motlagh, M. M. Kim, A. J. Minn, J. F. Dorsey, J. B . Foster, J. Metz, C. Koumenis, D. G. Kirsch, Y. Gong, and Y. Fan. F lash radiation reprograms lipid metabolism and macrophage immunity and sensitizes medullo...
2025
-
[24]
Geirnaert, L
F. Geirnaert, L. Kerkhove, P. Montay-Gruel, T. Gevaert, I. Dufait, and M. De Ridder. Exploring the metabolic impact of flash radiotherapy. Cancers, 17(1):133, 2025
2025
-
[25]
M. M. Kim, E. S. Diffenderfer, L. Lin, et al. Ultra-high dose rate fl ash radiotherapy sparing of peripheral blood lymphocytes: A modeling a nd experimental study. Int. J. Radiat. Oncol. Biol. Phys. , 118(2):450–461, 2024
2024
-
[26]
Mayles, A
P. Mayles, A. Nahum, and J-C. Rosenwald. Handbook of radiotherapy physics: theory and practice . Taylor & Francis, 2007
2007
-
[27]
Gonz´ alez-Crespo, F
I. Gonz´ alez-Crespo, F. G´ omez, O. L´ opez Pouso, and J. Pa rdo- Montero. An in-silico study of conventional and FLASH radiotherap y iso-effectiveness: potential impact of radiolytic oxygen depletion o n tu- mor growth curves and tumor control probability. Phys. Med. Biol. , 69(21):215016, 2024
2024
-
[28]
Taylor, R
E. Taylor, R. P. Hill, and D. L´ etourneau. Modeling the impact of s pa- tial oxygen heterogeneity on radiolytic oxygen depletion during FLA SH radiotherapy. Phys. Med. Biol. , 67(11):115017, 2022
2022
-
[29]
H. Song, Y. Kim, and W. Sung. Modeling of the FLASH effect for ion beam radiation therapy. Physica Medica, 108:102553, 2023
2023
-
[30]
H. Zhu, J. Schuemann, Q. Zhang, and L. E. Gerweck. Modeling t he impact of tissue oxygen profiles and oxygen depletion parameter un cer- tainties on biological response and therapeutic benefit of FLASH. Med. Phys., 51:670–681, 2024
2024
-
[31]
J. Pardo-Montero and I. Gonz´ alez-Crespo. On the calculatio n of the radiobiological effect of radiolytic oxygen depletion in flash radiother apy. arXiv preprint arXiv:2602.20855 , 2026. xvi
-
[32]
hypoxic fraction
B. G. Wouters and J. M. Brown. Cells at intermediate oxygen leve ls can be more important than the “hypoxic fraction” in determining tumor response to fractionated radiotherapy. Radiat. Res. , 147(5):541–550, 1997
1997
-
[33]
J. T. Lyman. Complication probability as assessed from dose-vo lume histograms. Radiat. Res., 104(2s):S13–S19, 1985
1985
-
[34]
G. J. Kutcher and C. Burman. Calculation of complication probab ility factors for non-uniform normal tissue irradiation: The effective v olume method. Int. J. Radiat. Oncol. Biol. Phys. , 16(6):1623–1630, 1989
1989
-
[35]
Niemierko
A. Niemierko. A generalized concept of equivalent uniform dose ( EUD). Med. Phys. , 26(6):1100, 1999
1999
-
[36]
S. F. Petit, A. L. A. J. Dekker, R. Seigneuric, L. Murrer, N. A. W. van Riel, M. Nordsmark, et al. Intra-voxel heterogeneity influenc es the dose prescription for dose-painting with radiotherapy: a mode lling study. Phys. Med. Biol. , 54(7):2179–2196, 2009
2009
-
[37]
Werner-Wasik, E
M. Werner-Wasik, E. Yorke, J. Deasy, J. Nam, and L. B. Marks . Radi- ation dose-volume effects in the esophagus. Int. J. Radiat. Oncol. Biol. Phys., 76(3):S86–S93, 2010
2010
-
[38]
Karsch, J
L. Karsch, J. Pawelke, M. Brand, S. Hans, K. Hidegh´ ety, J. J ansen, E. Lessmann, S. L¨ ock, M. Sch¨ urer, R. Schurig, et al. Beam pulse struc- ture and dose rate as determinants for the flash effect observed in ze- brafish embryo. Radiother. Oncol., 173:49–54, 2022
2022
-
[39]
K. Liu, T. Waldrop, E. Aguilar, N. Mims, D. Neill, A. Delahoussaye, Z. Li, D. Swanson, S. H Lin, A. C. Koong, et al. Redefining flash radiation therapy: the impact of mean dose rate and dose per pulse in the gastrointestinal tract. Int. J. Radiat. Oncol. Biol. Phys. , 121(4):1063– 1076, 2025. xvii
2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.