Recognition: unknown
Estimation of treatment effects in presence of differential use of post-randomization concomitant medication with time-to-event outcomes
Pith reviewed 2026-05-08 07:52 UTC · model grok-4.3
The pith
Causal estimands defined under time-dependent stochastic interventions isolate a randomized treatment's effect from differential post-randomization concomitant medication use in time-to-event trials.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The authors introduce a class of causal estimands that target the effect of the randomized treatment under time-dependent stochastic interventions that equalize the distribution of concomitant medication use across arms, thereby separating the specific impact of the study drug from the effects of additional therapies that arise more frequently in the control arm.
What carries the argument
Time-dependent stochastic interventions on concomitant medication use that balance exposure across randomized arms, estimated via targeted minimum loss-based estimation with adjustment for time-varying covariates.
If this is right
- Intention-to-treat estimates can be supplemented by quantities that remove dilution caused by extra medications started more often in the placebo arm.
- Treatment effects become comparable across trials that differ in their patterns of post-randomization medication use.
- Regulatory or clinical interpretations can focus on the isolated contribution of the study drug rather than the combined regimen that arises in practice.
- Estimation remains feasible under flexible time-dependent confounding adjustment without requiring deterministic interventions that would violate positivity.
Where Pith is reading between the lines
- The framework could be applied to re-analyze existing cardiovascular outcomes trials in diabetes to check whether reported benefits change once concomitant medication balance is enforced.
- Trials would benefit from collecting detailed time-stamped data on all concomitant medications to support these adjusted analyses.
- Similar stochastic balancing could address differential uptake of rescue therapies in other therapeutic areas such as oncology or infectious disease.
Load-bearing premise
That suitable stochastic rules exist which can balance concomitant medication exposure across arms while keeping positivity violations mild enough for the observed data to support valid estimation.
What would settle it
In a dataset where concomitant medication use is known to have no effect on the outcome, the new estimands should equal the standard intention-to-treat estimate; a large difference would indicate the method is not isolating the intended quantity.
Figures



read the original abstract
In placebo-controlled randomized trials, the post-randomization use of concomitant medications may be higher in the placebo arm than in the treatment arm. This may dilute the full benefits of the randomized drug as estimated by the intention-to-treat analysis. We focus on cardiovascular outcomes trials in type-2 diabetes patients of glucose-lowering treatments where patients in the placebo arm are more likely to add other glucose-lowering agents with established cardio-protective properties. As a supplement to the intention-to-treat analysis, we propose a class of estimands within a causal framework that isolates the specific impact of the treatment being studied from that of concomitant treatment use. These estimands are defined under time-dependent treatment interventions to balance exposure to additional medications across intervention arms. We advocate for specific stochastic interventions to achieve this balance while minimizing positivity violations, which arise when certain treatment combinations or characteristics are not sufficiently represented in the data. We employ targeted minimum loss-based estimation (TMLE) to optimize the estimation procedure for our estimands while allowing for flexible adjustments for time-dependent covariates from follow-up visits. Finally, we demonstrate the application of the methods through a simulation study and a real-world example from the LEADER cardiovascular outcomes trial, which assessed cardiovascular risk for liraglutide versus placebo.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes a class of causal estimands that isolate the effect of a randomized treatment (e.g., liraglutide) from differential post-randomization concomitant medication use in randomized trials with time-to-event outcomes. The estimands are defined via time-dependent stochastic interventions that re-sample concomitant medication histories to equalize exposure across arms while attempting to control positivity violations. Estimation proceeds via TMLE with flexible adjustment for time-varying covariates, and the approach is illustrated in a simulation study plus re-analysis of the LEADER cardiovascular outcomes trial.
Significance. If the identification and estimation results hold, the work supplies a principled supplement to standard ITT analyses for CVOTs in type-2 diabetes, where placebo-arm patients frequently initiate additional glucose-lowering agents. The use of TMLE and explicit stochastic interventions offers a transparent way to handle time-dependent confounding and differential concomitant use, which is a recurring practical issue in such trials.
major comments (3)
- [§3] §3 (stochastic intervention definition): the paper selects a specific intervention kernel to balance concomitant use while 'minimizing positivity violations,' but provides neither a formal proof that the intervened conditional density is positive on the support of the observed data process nor empirical diagnostics (e.g., minimum estimated propensity weights across time-varying covariate histories). Without this, the efficient influence function is not guaranteed to be well-defined and TMLE consistency is not assured under realistic time-dependent confounding.
- [§5] §5 (LEADER application): the manuscript reports results from the LEADER trial but does not detail the exact rules for handling missing time-varying covariate data, the number of patients excluded due to insufficient follow-up, or sensitivity analyses that vary the stochastic intervention parameter. These choices directly affect whether the reported point estimates and confidence intervals can be interpreted as isolating the liraglutide effect net of concomitant use.
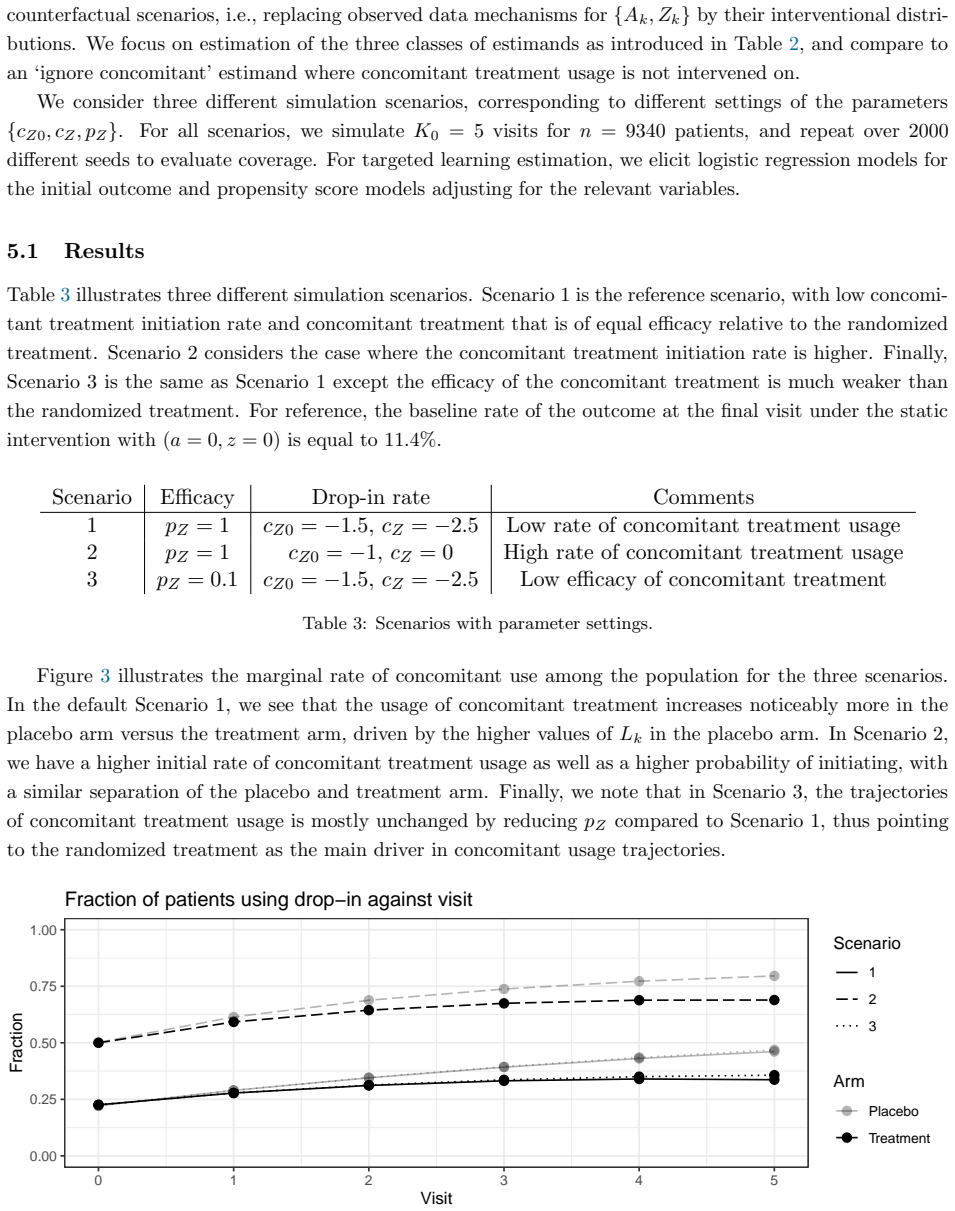
- [§4] §4 (simulation design): the simulation scenarios do not include cases in which the observed data process approaches positivity violation for certain covariate histories (e.g., extreme glucose trajectories that strongly predict concomitant medication). Consequently, the reported finite-sample performance does not test the robustness claim that the advocated interventions 'minimize' positivity problems.
minor comments (3)
- [Abstract] The abstract states that the methods are 'demonstrated' via simulation and LEADER but supplies no numerical summaries (bias, coverage, or hazard ratios); adding one sentence with key quantitative findings would improve readability.
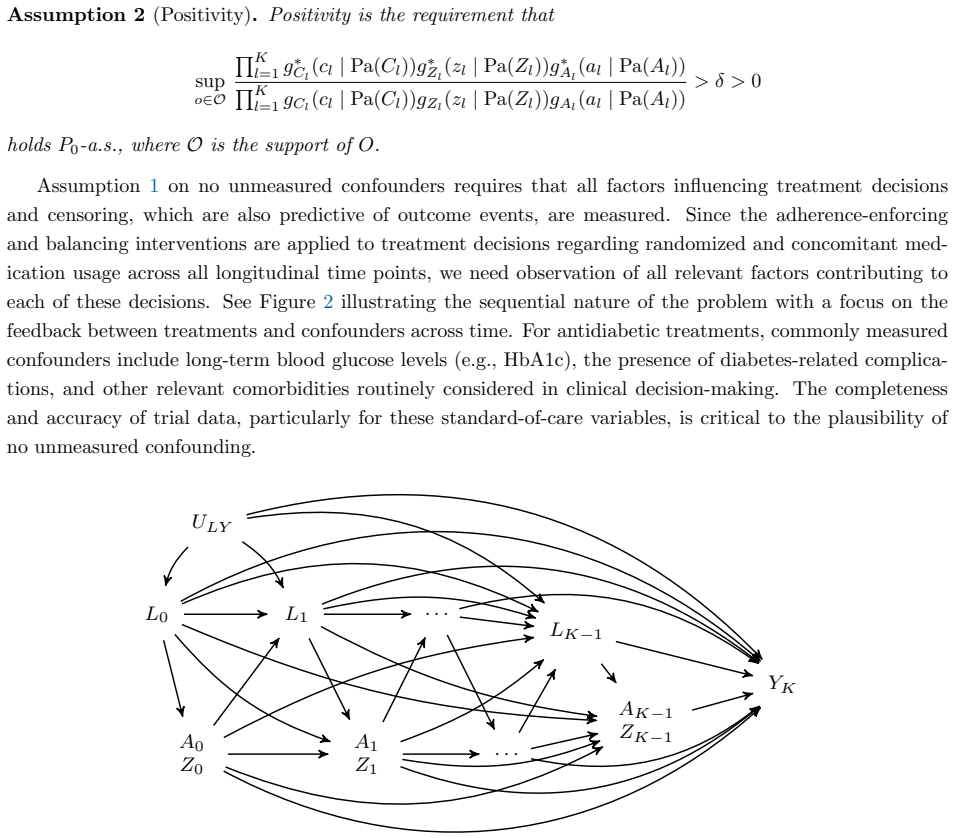
- [§2] Notation for the time-dependent treatment and covariate processes (e.g., A(t), L(t)) is introduced without an accompanying timeline diagram or concrete example of a patient history; this would clarify the intervention definition for readers unfamiliar with longitudinal causal inference.
- [§1] The paper cites standard TMLE references but does not compare the proposed estimands to existing approaches for handling post-randomization treatments (e.g., principal stratification or g-methods with deterministic interventions); a short paragraph situating the contribution would help.
Simulated Author's Rebuttal
We thank the referee for their insightful and constructive comments on our manuscript. We address each major comment point by point below, providing clarifications and indicating where revisions will be made to strengthen the paper.
read point-by-point responses
-
Referee: [§3] §3 (stochastic intervention definition): the paper selects a specific intervention kernel to balance concomitant use while 'minimizing positivity violations,' but provides neither a formal proof that the intervened conditional density is positive on the support of the observed data process nor empirical diagnostics (e.g., minimum estimated propensity weights across time-varying covariate histories). Without this, the efficient influence function is not guaranteed to be well-defined and TMLE consistency is not assured under realistic time-dependent confounding.
Authors: We appreciate this observation. The stochastic intervention is defined by resampling concomitant medication histories from the pooled observed data conditional on baseline covariates and time-varying factors, which ensures that the support of the intervened distribution is a subset of the observed support, thereby satisfying positivity by construction. However, we acknowledge the value of explicit verification and will include in the revision both a formal argument for positivity preservation and empirical diagnostics such as the minimum estimated weights over time-varying histories in both the simulation and LEADER analyses. revision: yes
-
Referee: [§5] §5 (LEADER application): the manuscript reports results from the LEADER trial but does not detail the exact rules for handling missing time-varying covariate data, the number of patients excluded due to insufficient follow-up, or sensitivity analyses that vary the stochastic intervention parameter. These choices directly affect whether the reported point estimates and confidence intervals can be interpreted as isolating the liraglutide effect net of concomitant use.
Authors: We agree that these details are important for interpretability. In the revised manuscript, we will expand the LEADER section to specify the missing data handling procedures (last observation carried forward with sensitivity checks), report the exact number of patients excluded for insufficient follow-up, and present sensitivity analyses for different values of the stochastic intervention parameter. This will strengthen the transparency of the application. revision: yes
-
Referee: [§4] §4 (simulation design): the simulation scenarios do not include cases in which the observed data process approaches positivity violation for certain covariate histories (e.g., extreme glucose trajectories that strongly predict concomitant medication). Consequently, the reported finite-sample performance does not test the robustness claim that the advocated interventions 'minimize' positivity problems.
Authors: The current simulations were calibrated to mimic the observed confounding structure in the LEADER trial without extreme violations. We recognize that testing near-positivity-violation scenarios would better support the robustness claim. We will add such scenarios to the simulation study in the revision, including performance metrics under these conditions to demonstrate the method's behavior when positivity is approached. revision: yes
Circularity Check
No significant circularity in estimand definition or TMLE application
full rationale
The paper defines new causal estimands under time-dependent stochastic interventions on concomitant medication to isolate treatment effects, then applies standard TMLE for estimation with time-varying covariate adjustment. These definitions and the use of TMLE (an established method) do not reduce by construction to fitted inputs, self-citations, or renamings within the paper. Identification relies on general causal assumptions and positivity conditions stated explicitly, with simulation and LEADER trial application serving as external checks rather than tautological confirmation. No load-bearing steps equate outputs to inputs via definition or prior self-work.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Standard causal assumptions (consistency, conditional exchangeability, positivity) hold for the defined time-dependent stochastic interventions
Reference graph
Works this paper leans on
-
[1]
Bang and J
H. Bang and J. M. Robins. Doubly robust estimation in missing data and causal inference models. Biometrics, 61 0 (4): 0 962--973, 2005
2005
-
[2]
M. A. Bethel, S. R. Stevens, J. B. Buse, J. Choi, S. M. Gustavson, N. Iqbal, Y. Lokhnygina, R. J. Mentz, R. A. Patel, and P. \"O hman. Exploring the possible impact of unbalanced open-label drop-in of glucose-lowering medications on exscel outcomes. Circulation, 141 0 (17): 0 1360--1370, 2020
2020
-
[3]
Didelez, P
V. Didelez, P. Dawid, and S. Geneletti. Direct and indirect effects of sequential treatments. Proceedings of the 22nd Annual Conference on Uncertainty in Artifical Intelligence, pages 138--146, 2006
2006
-
[4]
R. D. Gill and J. M. Robins. Causal inference for complex longitudinal data: the continuous case. Annals of Statistics, pages 1785--1811, 2001
2001
-
[5]
M. A. Hern \'a n. The hazards of hazard ratios. Epidemiology (Cambridge, Mass.), 21 0 (1): 0 13, 2010
2010
-
[6]
M. A. Hernan and J. Robins. Causal inference: What if. boca raton: Chapman & hill/crc. 2020
2020
-
[7]
M. A. Hern \'a n and J. M. Robins. Using big data to emulate a target trial when a randomized trial is not available. American journal of epidemiology, 183 0 (8): 0 758--764, 2016
2016
-
[8]
Addendum on estimands and sensitivity analysis in clinical trials to the guideline on statistical principles for clinical trials E 9 ( R 1)
ICH. Addendum on estimands and sensitivity analysis in clinical trials to the guideline on statistical principles for clinical trials E 9 ( R 1). Fed Regist, pages 1--19, 2019
2019
-
[9]
S. D. Lendle, J. Schwab, M. L. Petersen, and M. J. v an d er Laan . ltmle : An R package implementing targeted minimum loss-based estimation for longitudinal data. Journal of Statistical Software, 81 0 (1): 0 1--21, 2017. doi:10.18637/jss.v081.i01
-
[10]
S. P. Marso, G. H. Daniels, K. Brown-Frandsen, P. Kristensen, J. F. E. Mann, M. A. Nauck, S. E. Nissen, S. Pocock, N. R. Poulter, and S. W. M. S. M. Z. B. B. R. M. B. J. B. Ravn, L. S. Liraglutide and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, 375 0 (4): 0 311--322, 2016
2016
-
[11]
Martinussen, S
T. Martinussen, S. Vansteelandt, and P. K. Andersen. Subtleties in the interpretation of hazard contrasts. Lifetime Data Analysis, 26: 0 833--855, 2020
2020
-
[12]
D. K. McGuire, D. D’Alessio, S. J. Nicholls, S. E. Nissen, J. S. Riesmeyer, I. Pavo, S. Sethuraman, C. R. Heilmann, J. J. Kaiser, and G. J. Weerakkody. Transitioning to active-controlled trials to evaluate cardiovascular safety and efficacy of medications for type 2 diabetes. Cardiovascular Diabetology, 21 0 (1): 0 1--9, 2022
2022
-
[13]
Michiels, C
H. Michiels, C. Sotto, A. Vandebosch, and S. Vansteelandt. A novel estimand to adjust for rescue treatment in randomized clinical trials. Statistics in Medicine, 40 0 (9): 0 2257--2271, 2021
2021
-
[14]
J. Pearl. Direct and indirect effects. Proceedings of the seventeenth conference on uncertainty in artificial intelligence, pages 411--420, 2001
2001
-
[15]
Petersen, J
M. Petersen, J. Schwab, S. Gruber, N. Blaser, M. Schomaker, and M. v an d er Laan. Targeted maximum likelihood estimation for dynamic and static longitudinal marginal structural working models. Journal of causal inference, 2 0 (2): 0 147--185, 2014
2014
-
[16]
M. L. Petersen and M. J. van der Laan. Causal models and learning from data: integrating causal modeling and statistical estimation. Epidemiology (Cambridge, Mass.), 25 0 (3): 0 418, 2014
2014
-
[17]
M. L. Petersen, K. E. Porter, S. Gruber, Y. Wang, and M. J. van der Laan. Diagnosing and responding to violations in the positivity assumption. Statistical methods in medical research, 21 0 (1): 0 31--54, 2012
2012
-
[18]
E. C. Polley, S. Rose, and M. J. van der Laan. Super learning. In Targeted Learning, pages 43--66. Springer, 2011
2011
-
[19]
J. Robins. A new approach to causal inference in mortality studies with a sustained exposure period—application to control of the healthy worker survivor effect. Mathematical modelling, 7 0 (9-12): 0 1393--1512, 1986
1986
-
[20]
J. M. Robins and S. Greenland. Identifiability and exchangeability for direct and indirect effects. Epidemiology, pages 143--155, 1992
1992
-
[21]
O. M. Stitelman, V. De Gruttola, C. W. Wester, and M. J. van der Laan. Rcts with time-to-event outcomes and effect modification parameters. In Targeted Learning, pages 271--298. Springer, 2011
2011
-
[22]
M. J. v an d er Laan. A generally efficient targeted minimum loss based estimator based on the highly adaptive lasso. The International Journal of Biostatistics, 13 0 (2), 2017
2017
-
[23]
M. J. v an d er Laan and S. Gruber. Targeted minimum loss based estimation of causal effects of multiple time point interventions. The international journal of biostatistics, 8 0 (1), 2012
2012
-
[24]
M. J. van der Laan and M. L. Petersen. Direct effect models. The international journal of biostatistics, 4 0 (1), 2008
2008
-
[25]
M. J. v an d er Laan and S. Rose. Targeted learning: causal inference for observational and experimental data. Springer Science & Business Media, 2011
2011
-
[26]
M. J. v an d er Laan and S. Rose. Targeted learning in data science: causal inference for complex longitudinal studies. Springer, 2018
2018
-
[27]
M. J. v an d er Laan and D. Rubin. Targeted maximum likelihood learning. The International Journal of Biostatistics, 2 0 (1), 2006
2006
-
[28]
M. J. v an der Laan, E. C. Polley, and A. E. Hubbard. Super learner. Statistical applications in genetics and molecular biology, 6 0 (1), 2007
2007
-
[29]
T. J. VanderWeele and E. J. Tchetgen Tchetgen. Mediation analysis with time varying exposures and mediators. Journal of the Royal Statistical Society Series B: Statistical Methodology, 79 0 (3): 0 917--938, 2017
2017
-
[30]
Vansteelandt, M
S. Vansteelandt, M. Linder, S. Vandenberghe, J. Steen, and J. Madsen. Mediation analysis of time-to-event endpoints accounting for repeatedly measured mediators subject to time-varying confounding. Statistics in medicine, 38 0 (24): 0 4828--4840, 2019
2019
-
[31]
Zheng and M
W. Zheng and M. van der Laan. Longitudinal mediation analysis with time-varying mediators and exposures, with application to survival outcomes. Journal of causal inference, 5 0 (2), 2017
2017
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.