Recognition: 2 theorem links
· Lean TheoremHierarchical Perfusion Graphs for Tumor Heterogeneity Modeling in Glioma Molecular Subtyping
Pith reviewed 2026-05-11 02:21 UTC · model grok-4.3
The pith
A hierarchical graph neural network on perfusion codes from DSC-MRI predicts glioma molecular subtypes with high internal accuracy and external robustness without recalibration.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
HiPerfGNN first learns discrete hemodynamic representations from raw time-intensity curves using a vector-quantized variational autoencoder to define coarse-level graph nodes as functional tumor habitats; these nodes are then hierarchically subdivided into fine-level subregions guided by structural MRI, after which a hierarchical graph neural network propagates information across scales to predict molecular subtypes, reaching AUCs of 0.96 for IDH, 0.89 for 1p/19q codeletion, and 0.84 for WHO grade internally while maintaining 0.89 AUC for IDH externally.
What carries the argument
Hierarchical perfusion graph whose nodes are VQ-VAE-quantized perfusion codes representing tumor habitats, with structural-MRI-guided fine subdivisions and information flow via graph neural network layers.
If this is right
- Non-invasive subtyping can directly inform surgical planning and choice of chemotherapy or radiation without waiting for tissue results.
- Perfusion dynamics supply hemodynamic signatures that improve radiogenomic accuracy beyond what static anatomical MRI alone achieves.
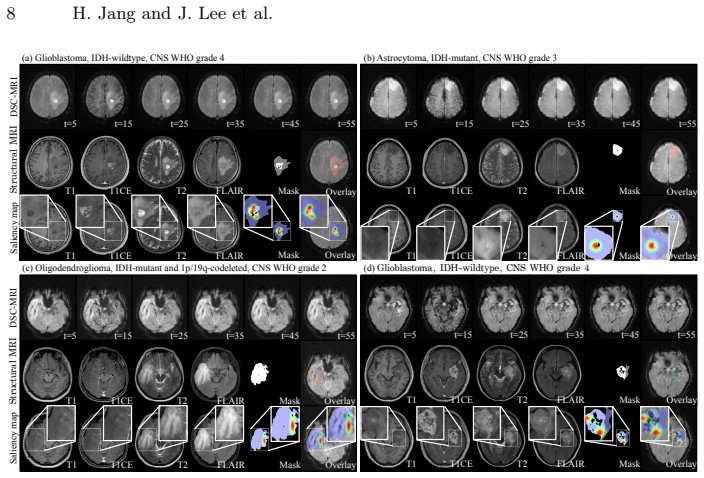
- Gradient saliency maps highlight regions consistent with known glioma vascular biology, providing a check on whether the model attends to plausible physiology.
- Robust external performance without recalibration indicates the framework can transfer to new hospitals using different scanners.
Where Pith is reading between the lines
- The same quantization-plus-hierarchy pattern could be tested on other dynamic-contrast modalities or tumor types where habitat heterogeneity matters.
- If the learned habitats prove stable across patients, they might serve as imaging biomarkers for monitoring treatment response rather than only initial subtyping.
- Adding a third scale or fusing additional sequences such as diffusion or spectroscopy could be evaluated to see whether multi-class grade prediction improves beyond the current 0.84 AUC.
Load-bearing premise
The discrete perfusion codes match biologically distinct tumor regions whose hierarchical arrangement lets the graph network separate molecular subtypes across different scanning sites.
What would settle it
A controlled experiment on the same cohorts in which replacing the learned VQ-VAE perfusion codes with random labels while preserving graph structure and structural MRI yields statistically indistinguishable AUCs would show that the hemodynamic discretization is not carrying the claimed signal.
Figures

read the original abstract
Precise molecular subtyping of gliomas, including isocitrate dehydrogenase (IDH) mutation and 1p/19q codeletion, directly guides surgical and therapeutic decisions, yet currently relies on invasive tissue sampling. Deep learning on structural MRI has emerged as a non-invasive alternative, but anatomy-only approaches cannot capture the hemodynamic signatures that distinguish molecular subtypes. Radiogenomics based on dynamic susceptibility contrast (DSC) MRI holds immense potential for non-invasively characterizing glioma molecular subtypes, yet clinical deployment has been hindered by inter-site variability and the limitations of voxel-wise analysis. We introduce HiPerfGNN, a framework that first learns discrete hemodynamic representations from raw time-intensity curves using a vector-quantized variational autoencoder (VQ-VAE). These quantized perfusion codes define coarse-level graph nodes representing functional tumor habitats, each of which is hierarchically subdivided into fine-level subregions guided by structural MRI. A hierarchical graph neural network then propagates information across scales for molecular prediction. On an internal cohort (n=475), the model achieved AUCs of 0.96 (IDH), 0.89 (1p/19q), and 0.84 (WHO grade), and maintained robust IDH performance (AUC 0.89) on an independent external cohort (n=397) without recalibration. Gradient-based saliency analysis confirms biologically grounded attention patterns aligned with known glioma pathophysiology. Our results demonstrate the added value of integrating perfusion dynamics into radiogenomic pipelines for glioma molecular subtyping. Code is available at https://github.com/janghana/HiPerfGNN.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript introduces HiPerfGNN, a framework for non-invasive glioma molecular subtyping from DSC-MRI. It uses a VQ-VAE to learn discrete perfusion codes from time-intensity curves, defines hierarchical graphs with coarse tumor habitats subdivided by structural MRI, and applies a GNN to predict IDH mutation status, 1p/19q codeletion, and WHO grade. Strong AUCs are reported on an internal cohort (n=475): 0.96 (IDH), 0.89 (1p/19q), 0.84 (grade); IDH AUC remains 0.89 on an independent external cohort (n=397) without recalibration. Saliency maps are shown to align with known pathophysiology, and code is released.
Significance. If the external generalization claim holds after addressing transferability, the work demonstrates that perfusion-derived discrete codes and hierarchical GNN modeling can improve radiogenomic prediction over anatomy-only methods while mitigating some inter-site variability. Code release supports reproducibility and enables follow-up studies on hemodynamic habitat modeling.
major comments (3)
- [Methods (VQ-VAE and external evaluation)] Methods (VQ-VAE training and inference): The VQ-VAE codebook is learned exclusively on the internal cohort. For external validation the same fixed codebook is applied without adaptation or retraining. Site-specific differences in contrast timing, scanner field strength, or acquisition parameters can shift the distribution of time-intensity curves, altering which code indices are assigned to equivalent hemodynamic states. The manuscript must supply direct evidence (e.g., code-frequency histograms, reconstruction MSE, or t-SNE embeddings of external vs. internal curves) that the discrete codes remain semantically consistent across sites; without it the reported AUC 0.89 on the external cohort rests on an untested invariance assumption.
- [Results and Experimental Setup] Results and experimental protocol: The abstract and results sections state high AUCs on sizable cohorts yet omit patient-level data-split details (train/val/test ratios, stratification by site or grade), DSC-MRI preprocessing pipeline (normalization, motion correction, arterial input function selection), hyperparameter search procedure, and any statistical testing (DeLong test, bootstrap CIs) for the reported AUC differences. These omissions make it impossible to judge whether the performance numbers are robust or overfit to the internal cohort.
- [Methods (Graph Construction) and Ablation Studies] Hierarchical graph construction: The claim that coarse VQ-VAE codes define biologically distinct habitats whose fine-level subdivision improves subtype discrimination is central to the architecture. The manuscript should quantify the contribution of the hierarchy (e.g., ablation removing the fine-level nodes or the GNN message passing across scales) and show that the performance gain is not simply due to increased model capacity.
minor comments (2)
- [Results (Saliency Analysis)] Figure captions and saliency analysis: The gradient-based saliency maps are described as 'biologically grounded,' but the exact attribution method (e.g., Grad-CAM variant, integrated gradients) and the quantitative overlap metric with known glioma regions are not stated. Adding these details would strengthen interpretability claims.
- [Methods (Hierarchical GNN)] Notation: The distinction between 'coarse-level graph nodes' and 'fine-level subregions' is introduced without an accompanying diagram or equation defining the two-scale adjacency matrices; a small schematic would clarify the hierarchical message-passing scheme.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed feedback on our manuscript. We address each major comment point-by-point below, providing clarifications and indicating the revisions we will incorporate to strengthen the work.
read point-by-point responses
-
Referee: Methods (VQ-VAE and external evaluation): The VQ-VAE codebook is learned exclusively on the internal cohort. For external validation the same fixed codebook is applied without adaptation or retraining. Site-specific differences in contrast timing, scanner field strength, or acquisition parameters can shift the distribution of time-intensity curves, altering which code indices are assigned to equivalent hemodynamic states. The manuscript must supply direct evidence (e.g., code-frequency histograms, reconstruction MSE, or t-SNE embeddings of external vs. internal curves) that the discrete codes remain semantically consistent across sites; without it the reported AUC 0.89 on the external cohort rests on an untested invariance assumption.
Authors: We agree that demonstrating semantic consistency of the VQ-VAE codes across sites is essential to support the external generalization claim. In the revised manuscript, we will add code-frequency histograms comparing the internal and external cohorts, t-SNE embeddings of time-intensity curves from both sites (colored by assigned code indices), and the reconstruction MSE achieved on the external data using the fixed codebook. These visualizations and metrics will provide direct evidence that the discrete representations capture equivalent hemodynamic states despite site differences, thereby justifying the reported AUC without site-specific adaptation. revision: yes
-
Referee: Results and experimental protocol: The abstract and results sections state high AUCs on sizable cohorts yet omit patient-level data-split details (train/val/test ratios, stratification by site or grade), DSC-MRI preprocessing pipeline (normalization, motion correction, arterial input function selection), hyperparameter search procedure, and any statistical testing (DeLong test, bootstrap CIs) for the reported AUC differences. These omissions make it impossible to judge whether the performance numbers are robust or overfit to the internal cohort.
Authors: We acknowledge that the experimental protocol details require greater explicitness for full reproducibility assessment. The full manuscript Methods section already specifies the stratified 70/15/15 train/validation/test splits (by molecular subtype, grade, and site), DSC-MRI preprocessing (including z-score normalization, motion correction, and AIF selection), and grid-search hyperparameter tuning. To address the concern directly, we will expand these descriptions in the main text, add bootstrap-derived 95% CIs for all AUCs, and include DeLong tests comparing our model against baselines. A new supplementary table will tabulate all protocol parameters. revision: yes
-
Referee: Hierarchical graph construction: The claim that coarse VQ-VAE codes define biologically distinct habitats whose fine-level subdivision improves subtype discrimination is central to the architecture. The manuscript should quantify the contribution of the hierarchy (e.g., ablation removing the fine-level nodes or the GNN message passing across scales) and show that the performance gain is not simply due to increased model capacity.
Authors: We concur that ablation studies are needed to isolate the benefit of the hierarchical design from mere capacity increases. In the revised manuscript, we will add a dedicated ablation table reporting performance on both internal and external cohorts for: (i) the full hierarchical model, (ii) a coarse-only flat graph, (iii) a hierarchical model without cross-scale message passing, and (iv) a capacity-matched non-hierarchical GNN baseline with equivalent parameter count. These results will quantify the incremental value of fine-level subdivision and multi-scale propagation while controlling for capacity, and will be discussed in relation to tumor habitat heterogeneity. revision: yes
Circularity Check
No significant circularity; external-cohort AUCs are genuine held-out evaluation
full rationale
The paper trains the VQ-VAE, hierarchical graph construction, and GNN on an internal cohort (n=475) and reports AUCs on a completely separate external cohort (n=397) without recalibration or parameter reuse. No equations or procedures in the abstract or described pipeline reduce the reported performance metrics to quantities defined by the same fitted parameters. The discrete perfusion codes are learned from internal time-intensity curves, but the external evaluation constitutes an independent test of transfer; any domain-shift risk is an empirical robustness question, not a definitional or self-citation reduction. Minor self-citation (if present in the full text) is not load-bearing for the central claim.
Axiom & Free-Parameter Ledger
free parameters (1)
- VQ-VAE codebook size
axioms (1)
- domain assumption Perfusion dynamics contain information that distinguishes IDH, 1p/19q, and grade status
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
VQ-VAE ... quantized perfusion codes define coarse-level graph nodes ... hierarchical graph neural network ... PNA layers with multiple aggregators
-
IndisputableMonolith/Foundation/AbsoluteFloorClosure.leanabsolute_floor_iff_bare_distinguishability unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
K=2, N=3, d_enc=256 ... LVQ = ||x-x̂||1 + commitment loss
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
IEEE Transactions on Pattern Analysis and Machine Intelligence34(11), 2274–2282 (2012)
Achanta, R., Shaji, A., Smith, K., Lucchi, A., Fua, P., Süsstrunk, S.: SLIC su- perpixels compared to state-of-the-art superpixel methods. IEEE Transactions on Pattern Analysis and Machine Intelligence34(11), 2274–2282 (2012)
work page 2012
-
[2]
Nature Commu- nications5(1), 4006 (2014)
Aerts, H.J., Velazquez, E.R., Leijenaar, R.T., et al.: Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nature Commu- nications5(1), 4006 (2014)
work page 2014
-
[3]
Radiol- ogy287(3), 933–943 (2018)
Anzalone, N., et al.: Brain gliomas: multicenter standardized assessment of dy- namic contrast-enhanced and dynamic susceptibility contrast mr images. Radiol- ogy287(3), 933–943 (2018)
work page 2018
-
[4]
Journal of Magnetic Resonance Imaging 47(4), 915–924 (2018)
Artzi, M., Bressler, I., Ben Bashat, D.: Deciphering glioma genetics following ra- diogenomics analysis of MR perfusion. Journal of Magnetic Resonance Imaging 47(4), 915–924 (2018)
work page 2018
-
[5]
Bakas, S., Reyes, M., Jakab, A., Bauer, S., Rempfler, M., Crimi, A., Shinohara, R.T., Berger, C., Ha, S.M., Rozycki, M., et al.: Identifying the best machine learn- ing algorithms for brain tumor segmentation, progression assessment, and overall survival prediction in the brats challenge. arXiv preprint arXiv:1811.02629 (2018)
work page Pith review arXiv 2018
-
[6]
Rudie, Nazím Flores Santamaría, Anahita Fathi Kazerooni, Sarthak Pati, et al
Bakas, S., Sako, C., Akbari, H., et al.: The university of pennsylvania glioblastoma (upenn-gbm) cohort: advanced mri, clinical, genomics, & radiomics. Scientific Data 9(1) (2022).https://doi.org/10.1038/s41597-022-01560-7 10 H. Jang and J. Lee et al
-
[7]
IEEE Transactions on Medical Imaging44, 101–112 (2025)
Byeon, H., Lee, S., Kim, J., et al.: GlioMT: A multimodal vision transformer for glioma subtyping. IEEE Transactions on Medical Imaging44, 101–112 (2025)
work page 2025
-
[8]
In: International Conference on Machine Learning
Cai, T., Luo, S., Xu, K., He, D., Liu, T.y., Wang, L.: Graphnorm: A principled ap- proach to accelerating graph neural network training. In: International Conference on Machine Learning. pp. 1204–1215. PMLR (2021)
work page 2021
-
[9]
Clinical Cancer Research24(5), 1073–1081 (2018)
Chang, K., Bai, H.X., Zhou, H., Su, C., Bi, W.L., Agbodza, E., Kavouridis, V.K., Senders, J.T., Boaro, A., Beers, A., et al.: Residual convolutional neural network for the determination of idh status in low-and high-grade gliomas from mr imaging. Clinical Cancer Research24(5), 1073–1081 (2018)
work page 2018
-
[10]
Neuro-Oncology21(9), 1197–1209 (2019)
Choi, K.S., Bak, S.J., Ahn, S.S., et al.: Predicting IDH mutation using DSC-MRI and an explainable recurrent neural network. Neuro-Oncology21(9), 1197–1209 (2019)
work page 2019
-
[11]
Neuro-oncology 23(2), 304–313 (2021)
Choi, Y.S., Bae, S., Chang, J.H., Kang, S.G., Kim, S.H., Kim, J., Rim, T.H., Choi, S.H., Jain, R., Lee, S.K.: Fully automated hybrid approach to predict the idh mutation status of gliomas via deep learning and radiomics. Neuro-oncology 23(2), 304–313 (2021)
work page 2021
-
[12]
Advances in neural information processing systems33, 13260–13271 (2020)
Corso, G., Cavalleri, L., Beaini, D., Liò, P., Veličković, P.: Principal neighbourhood aggregation for graph nets. Advances in neural information processing systems33, 13260–13271 (2020)
work page 2020
-
[13]
In: International Conference on Medical Image Computing and Computer-Assisted Intervention
Farahani, S., Hejazi, M., Di Ieva, A., Liu, S.: Foundbionet: A foundation-based model for idh genotyping of glioma from multi-parametric mri. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. pp. 259–270. Springer (2025)
work page 2025
-
[14]
Radiology278(2), 563–577 (2016)
Gillies, R.J., Kinahan, P.E., Hricak, H.: Radiomics: images are more than pictures, they are data. Radiology278(2), 563–577 (2016)
work page 2016
-
[15]
The Lancet Oncology20(5), 728–740 (2019)
Kickingereder, P., Isensee, F., Tursunova, I., Petersen, J., Neuberger, U., Bonekamp, D., Brugnara, G., Schell, M., Kessler, T., Foltyn, M., et al.: Automated quantitative tumour response assessment of mri in neuro-oncology with artificial neural networks: a multicentre, retrospective study. The Lancet Oncology20(5), 728–740 (2019)
work page 2019
-
[16]
Scientific reports5(1), 16238 (2015)
Kickingereder, P., Sahm, F., Radbruch, A., Wick, W., Heiland, S., Deimling, A.v., Bendszus, M., Wiestler, B.: Idh mutation status is associated with a distinct hypoxia/angiogenesis transcriptome signature which is non-invasively predictable with rcbv imaging in human glioma. Scientific reports5(1), 16238 (2015)
work page 2015
-
[17]
Radiology290(1), 194–202 (2019)
Kickingereder, P., et al.: Radiomic profiling of glioblastoma: identifying an imaging predictor of patient survival with improved performance over established clinical and radiologic risk models. Radiology290(1), 194–202 (2019)
work page 2019
-
[18]
Semi-Supervised Classification with Graph Convolutional Networks
Kipf, T.: Semi-supervised classification with graph convolutional networks. arXiv preprint arXiv:1609.02907 (2016)
work page internal anchor Pith review Pith/arXiv arXiv 2016
-
[19]
Radiology247(2), 490–498 (2008)
Law, M., Young, R.J., Babb, J.S., et al.: Glioma grading: sensitivity, specificity, and predictive values of perfusion MR imaging. Radiology247(2), 490–498 (2008)
work page 2008
-
[20]
Neuro-oncology16(2), 297–305 (2014)
Leu, K., Ott, G., Lai, A., et al.: Relative cerebral blood volume is a marker for stratification of fair prognosis in IDH1-mutated WHO grade II and III astrocy- tomas. Neuro-oncology16(2), 297–305 (2014)
work page 2014
-
[21]
Acta Neuropathologica142, 11–28 (2021)
Louis, D.N., Perry, A., Wesseling, P., et al.: The 2021 WHO classification of tu- mours of the central nervous system: a summary. Acta Neuropathologica142, 11–28 (2021)
work page 2021
-
[22]
Van den Oord, A., Vinyals, O., Kavukcuoglu, K.: Neural discrete representation learning.In:AdvancesinNeuralInformationProcessingSystems.vol.30,pp.6306– 6315 (2017) HiPerfGNN 11
work page 2017
-
[23]
Medical Image Analysis75, 102264 (2022)
Pati, P., et al.: Hierarchical graph representations in digital pathology. Medical Image Analysis75, 102264 (2022)
work page 2022
-
[24]
In: Proceedings of the IEEE/CVF conference on computer vision and pattern recognition
Pope, P.E., Kolouri, S., Rostami, M., Martin, C.E., Hoffmann, H.: Explainabil- ity methods for graph convolutional neural networks. In: Proceedings of the IEEE/CVF conference on computer vision and pattern recognition. pp. 10772– 10781 (2019)
work page 2019
-
[25]
Nature Reviews Neurology17(8), 486–500 (2021)
Smits, M.: Mri biomarkers in neuro-oncology. Nature Reviews Neurology17(8), 486–500 (2021)
work page 2021
-
[26]
Nature reviews Clinical oncology18(3), 170–186 (2021)
Weller, M., van den Bent, M., Preusser, M., Le Rhun, E., Tonn, J.C., Minniti, G., Bendszus, M., Balana, C., Chinot, O., Dirven, L., et al.: Eano guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nature reviews Clinical oncology18(3), 170–186 (2021)
work page 2021
-
[27]
New England Journal of Medicine359(5), 492–507 (2008)
Wen, P.Y., Kesari, S.: Malignant gliomas in adults. New England Journal of Medicine359(5), 492–507 (2008)
work page 2008
-
[28]
In: International conference on machine learning
Xu, K., Li, C., Tian, Y., Sonobe, T., Kawarabayashi, K.i., Jegelka, S.: Repre- sentation learning on graphs with jumping knowledge networks. In: International conference on machine learning. pp. 5453–5462. pmlr (2018)
work page 2018
-
[29]
In: Medical Image Computing and Computer Assisted Intervention–MICCAI 2024
Yan, Z., Wang, S., Huang, R., et al.: PerfGAT: spatiotemporal graph attention networks for perfusion MRI radiogenomics. In: Medical Image Computing and Computer Assisted Intervention–MICCAI 2024. pp. 123–133. Springer (2024)
work page 2024
-
[30]
Zacharaki, E.I., Wang, S., Chawla, S., Soo Yoo, D., Wolf, R., Melhem, E.R., Da- vatzikos, C.: Classification of brain tumor type and grade using mri texture and shape in a machine learning scheme. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine62(6), 1609–1618 (2009)
work page 2009
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.