Recognition: no theorem link
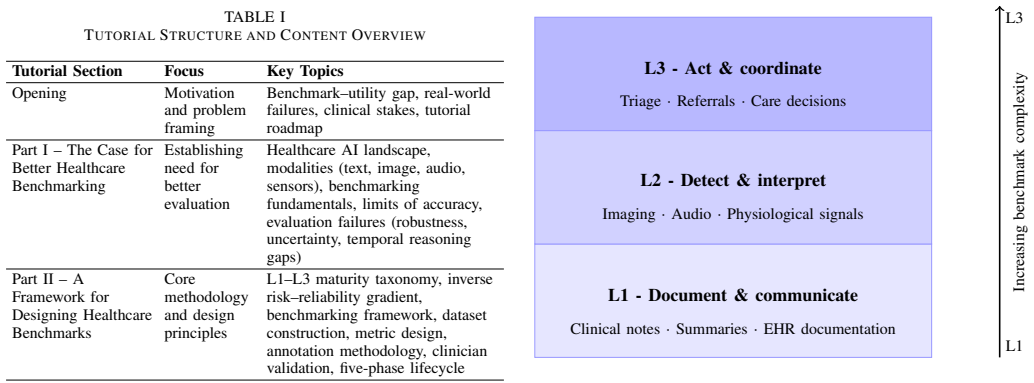
Measuring What Matters: Benchmarking Generative, Multimodal, and Agentic AI in Healthcare
Pith reviewed 2026-05-12 01:22 UTC · model grok-4.3
The pith
High benchmark scores on medical exams give a false sense of readiness for AI in real clinical settings.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The paper establishes that the central challenge in healthcare AI is not raw performance but the lack of systematic methods to measure reliability, safety, and clinical relevance under real-world conditions. Existing benchmarks test knowledge but not dependable execution across the complexity of clinical tasks, resulting in a widening gap between benchmark results and actual utility as systems assume more responsibility.
What carries the argument
The mismatch between high scores on ad hoc knowledge benchmarks and degraded performance on real clinical tasks like documentation and decision support.
If this is right
- Adopting better benchmarks would reveal where models truly fall short in clinical environments.
- Deployment decisions could be based on measured utility rather than exam scores.
- The field would gain reproducible ways to compare models on safety and relevance.
- Research could shift toward improving performance on the harder, more consequential tasks.
Where Pith is reading between the lines
- Such benchmarks might show that generative and agentic systems require new training paradigms focused on workflow integration.
- Similar issues likely appear in other high-stakes domains where benchmarks lag behind application complexity.
- A practical test would involve creating workflow-based benchmarks and checking if they better correlate with outcomes in pilot deployments.
Load-bearing premise
That the sharp drops in performance on real tasks are caused by inadequate benchmark design more than by the models themselves being unable to handle clinical complexity.
What would settle it
If new benchmarks designed to mirror full clinical workflows still show the same high scores as exam benchmarks, that would indicate the performance gap is not due to benchmark flaws.
Figures
read the original abstract
AI models are increasingly deployed in live clinical environments where they must perform reliably across complex, high-stakes workflows that standard training and validation datasets were never designed to capture. Evaluating these systems requires benchmarks: structured combinations of tasks, datasets, and metrics that enable reproducible, comparable measurement of what a model can do. The central challenge in healthcare AI is not performance alone, but the absence of systematic methods to measure reliability, safety, and clinical relevance under real-world conditions. Most existing benchmarks test what a model knows; too few test whether it can perform reliably and without failing across the full complexity of real clinical tasks. Current benchmarks have accumulated through ad hoc dataset construction optimized for narrow task performance: frontier models achieve near-perfect scores on medical licensing examinations, but when evaluated across real clinical tasks, performance degrades sharply, scoring 0.74--0.85 on documentation, 0.61--0.76 on clinical decision support, and only 0.53--0.63 on administrative and workflow tasks \cite{medhelm}. High benchmark scores give a false sense of deployment readiness, and the gap between performance and utility widens precisely as AI systems take on more consequential clinical roles. Without a principled framework for benchmark design, the field cannot determine whether poor clinical performance reflects model limitations or failures in how performance is being measured.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript is a position paper arguing that current benchmarks for generative, multimodal, and agentic AI in healthcare are inadequate. Frontier models achieve near-perfect scores on medical licensing examinations, but performance degrades sharply on real clinical tasks (0.74-0.85 on documentation, 0.61-0.76 on clinical decision support, 0.53-0.63 on administrative and workflow tasks, per the cited MedHelm study). This creates a false sense of deployment readiness, with the gap between benchmark performance and clinical utility widening as AI assumes more consequential roles. The paper calls for a principled framework for benchmark design to measure reliability, safety, and relevance under real-world conditions, while noting uncertainty over whether poor clinical performance stems from model limitations or measurement failures.
Significance. If the cited performance gaps are shown to reflect genuine shortfalls in clinical utility rather than benchmark artifacts, the paper would usefully highlight a systemic evaluation challenge in healthcare AI. It could help steer the field toward benchmarks that better capture workflow complexity, supporting more reliable deployment decisions. The explicit acknowledgment of ambiguity between model and measurement issues is a constructive element that could prompt further methodological work.
major comments (1)
- [Abstract] Abstract (final sentence): The central claim asserts that high benchmark scores give a false sense of deployment readiness and that the gap widens on consequential clinical roles, supported by the cited score drops on real tasks. Yet the manuscript concedes that existing data leave open whether these low numbers reflect model limitations or 'failures in how performance is being measured.' No comparative validity evidence or criterion is supplied for treating the ad-hoc clinical datasets as closer to ground truth than licensing exams. This undercuts the load-bearing interpretation that the drops demonstrate unreadiness.
minor comments (2)
- [Abstract] The citation to MedHelm is invoked for the specific performance ranges but the full reference details are not visible in the provided text; ensure the bibliography entry is complete and accessible.
- [Abstract] The call for a 'principled framework' is stated at a high level; adding one or two concrete design principles or examples (e.g., criteria for task selection or validity checks) would make the recommendation more actionable without expanding scope.
Simulated Author's Rebuttal
We thank the referee for their constructive feedback on our position paper. We have addressed the concern regarding the abstract by revising the language to better reflect the acknowledged uncertainties in the data while preserving the core argument that current benchmarks are inadequate for assessing real-world clinical utility. We believe these changes improve the manuscript's precision.
read point-by-point responses
-
Referee: [Abstract] Abstract (final sentence): The central claim asserts that high benchmark scores give a false sense of deployment readiness and that the gap widens on consequential clinical roles, supported by the cited score drops on real tasks. Yet the manuscript concedes that existing data leave open whether these low numbers reflect model limitations or 'failures in how performance is being measured.' No comparative validity evidence or criterion is supplied for treating the ad-hoc clinical datasets as closer to ground truth than licensing exams. This undercuts the load-bearing interpretation that the drops demonstrate unreadiness.
Authors: We appreciate the referee pointing out this important nuance in our argument. As a position paper, we do not claim to have conducted a formal validation study comparing the two types of benchmarks; instead, we draw on the MedHelm study's design, which explicitly constructs tasks from real clinical workflows (e.g., generating discharge summaries from patient notes and supporting differential diagnosis in context), to argue that these better reflect the complexities of deployment than multiple-choice licensing exams. The concession in the manuscript is intentional to underscore the need for improved measurement frameworks rather than to weaken the claim. However, to address the concern directly, we have revised the abstract to state that high benchmark scores 'may give a false sense of deployment readiness' and have added a new paragraph in the discussion section calling for future research on benchmark validation criteria. This revision acknowledges the ambiguity while maintaining that the observed performance gaps highlight systemic issues in current evaluation practices. revision: yes
Circularity Check
No circularity: position paper with no derivations or self-referential reductions.
full rationale
The manuscript is a conceptual discussion of benchmarking challenges in healthcare AI. It contains no equations, derivations, fitted parameters, or self-citations that bear load on a central claim. Performance figures are attributed to an external citation (medhelm) and the text explicitly notes uncertainty about whether low clinical-task scores reflect model limits or measurement issues, without asserting one interpretation as ground truth or reducing any conclusion to its own inputs by construction. The argument is self-contained as an external-citation-supported position statement.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Existing benchmarks test knowledge but not reliable performance across the full complexity of real clinical tasks.
Reference graph
Works this paper leans on
-
[1]
Bedi, Suhana, et al. ”Medhelm: Holistic evaluation of large language models for medical tasks.” arXiv preprint arXiv:2505.23802 (2025)
-
[2]
Beyond the Leaderboard: Rethinking Medical Benchmarks for Large Language Models
Ma, Zizhan, et al. ”Beyond the leaderboard: Rethinking medical bench- marks for large language models.” arXiv preprint arXiv:2508.04325 (2025)
work page internal anchor Pith review Pith/arXiv arXiv 2025
-
[3]
Automating expert-level medical reasoning evaluation of large language models,
S. Zhouet al., “Automating expert-level medical reasoning evaluation of large language models,”Nature Machine Intelligence, vol. 7, no. 12, pp. 1102–1115, Dec. 2025, doi: 10.1038/s42256-025-07988-x
-
[4]
The Science of Benchmarking: What’s Measured, What’s Missing, What’s Next,
M. Z. Ma, M. Saxon, and X. Yue, “The Science of Benchmarking: What’s Measured, What’s Missing, What’s Next,” inProc. 39th Conf. Neural Information Processing Systems (NeurIPS) Tutorials, San Diego, CA, USA, Dec. 2025
work page 2025
- [5]
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.