Accurate Recognition of Pneumonia and COVID-19 by Geometric Shape Normalization of Lung Region using Automatic Landmark Detection and Piecewise Affine Warping
Pith reviewed 2026-06-30 06:47 UTC · model grok-4.3
The pith
Geometric normalization of lung shapes in chest X-rays improves COVID-19 and pneumonia classification by reducing acquisition artifacts.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
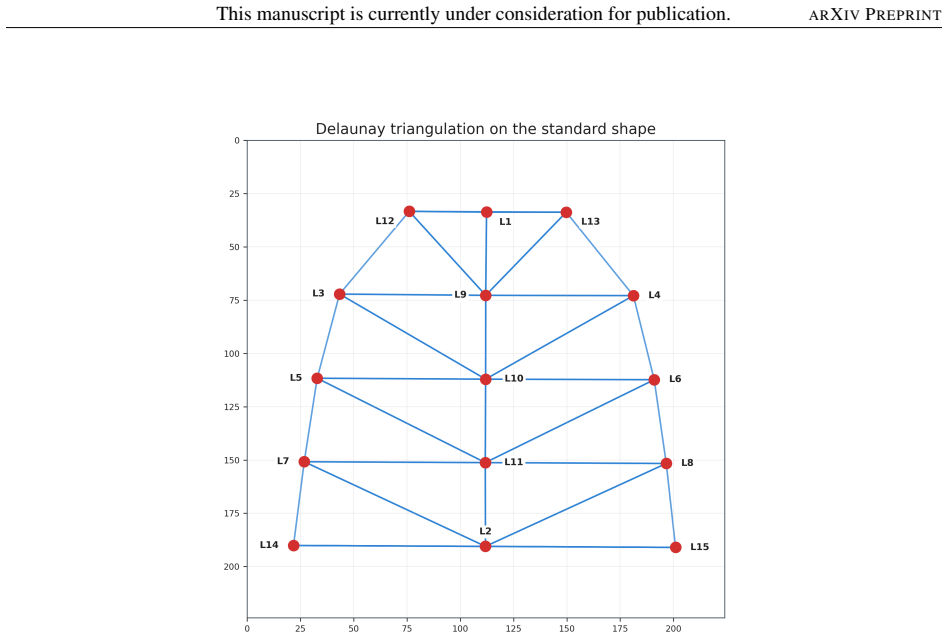
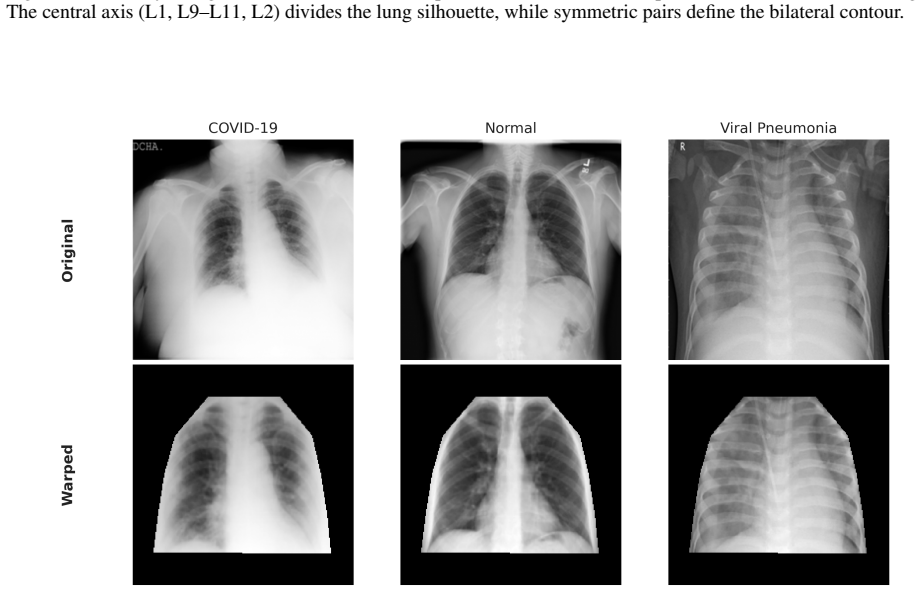
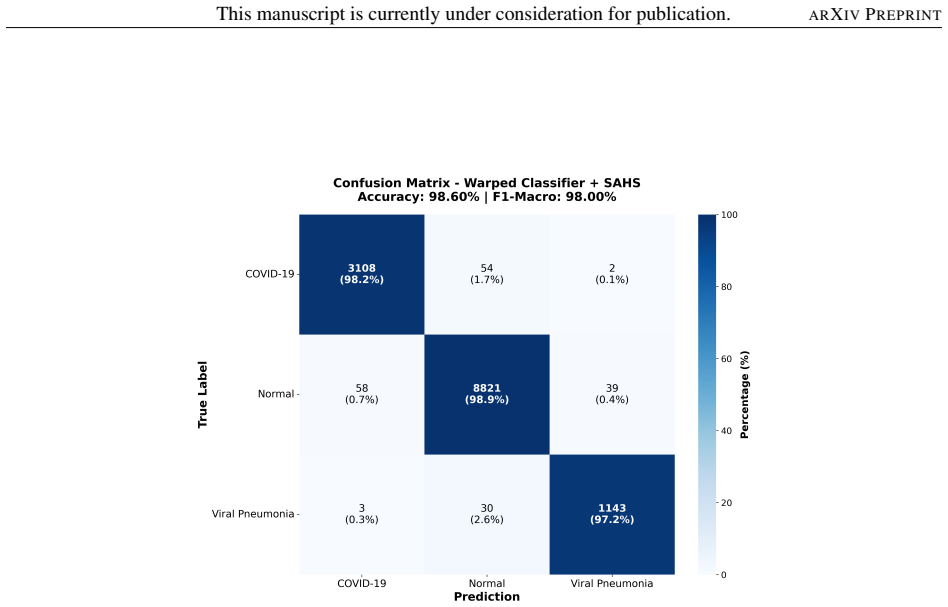
A ResNet-18 detector locates 15 lung-contour landmarks with 3.61-pixel mean error; these landmarks drive Generalized Procrustes Analysis, Delaunay triangulation, and piecewise affine warping that maps every lung region to one fixed shape. Classifiers trained on the resulting normalized images achieve 98.60 percent accuracy and 98.00 percent F1-macro on the COVID-19 Radiography Database under five-fold cross-validation and outperform artifact-masked unaligned images on both the original database (98.60 percent versus 96.24 percent) and a balanced adult-pediatric collection (94.67 percent versus 94.17 percent).
What carries the argument
Piecewise affine warping driven by 15 automatically detected lung-contour landmarks, which standardizes lung shape while preserving disease-relevant features for the downstream classifier.
If this is right
- Normalized images yield higher accuracy than artifact-masked or cropped unaligned versions on the COVID-19 Radiography Database.
- The same advantage appears on a balanced dataset that mixes adult and pediatric cases.
- Grad-CAM visualizations indicate the classifier relies less on acquisition artifacts when given normalized inputs.
- The landmark detector reaches 3.61-pixel mean error via an ensemble of four ResNet-18 models with test-time augmentation.
Where Pith is reading between the lines
- The same landmark-and-warp pipeline could be tested on other chest X-ray tasks such as tuberculosis or cardiomegaly detection to check whether shape standardization helps more broadly.
- If landmark detection error grows on lower-quality scans, the performance gain from normalization may shrink or reverse.
- Combining this geometric step with intensity-based augmentations might further stabilize classification across different scanners.
Load-bearing premise
The 15 predicted landmarks are accurate enough that the warping step removes shape variation without distorting the disease features the classifier needs.
What would settle it
A new test set in which all acquisition artifacts have already been removed by other means, showing that normalized images no longer outperform unaligned ones, would falsify the claim that normalization supplies an artifact-resistant representation.
Figures










read the original abstract
This paper presents an automatic system for recognizing pulmonary diseases in chest X-rays using geometric normalization of the lung region. The method combines three modules: (1) a ResNet-18 landmark detector with coordinate attention that predicts 15 lung-contour landmarks, achieving a mean localization error of 3.61 pixels through an ensemble of four models with test-time augmentation; (2) a geometric normalizer based on Generalized Procrustes Analysis, Delaunay triangulation, and piecewise affine warping to map each lung region to a standardized shape; and (3) a ResNet-18 classifier with transfer learning and SAHS contrast enhancement to classify images as COVID-19, Viral Pneumonia, or Normal. On the COVID-19 Radiography Database, the normalized-image classifier achieved 98.60+/-0.26% accuracy and 98.00% F1-Macro using five-fold cross-validation. Although original images produced slightly higher raw accuracy, Grad-CAM and cropping experiments suggest that this advantage is partly influenced by acquisition artifacts. In contrast, geometrically normalized images outperformed artifact-masked/cropped unaligned images on both the COVID-19 Radiography Database (98.60% vs. 96.24%) and a balanced adult-pediatric mixed dataset including pediatric cases from the Kermany dataset (94.67% vs. 94.17%). These results suggest that anatomical alignment can provide a more controlled and artifact-resistant representation for pulmonary disease recognition.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript describes an automatic system for pulmonary disease recognition in chest X-rays that detects 15 lung-contour landmarks using an ensemble of ResNet-18 models with coordinate attention (mean error 3.61 pixels), applies Generalized Procrustes Analysis, Delaunay triangulation, and piecewise affine warping for geometric normalization of the lung region, and then uses a ResNet-18 classifier with SAHS contrast enhancement. On the COVID-19 Radiography Database, normalized images achieve 98.60% accuracy in 5-fold CV, outperforming artifact-masked unaligned images (96.24%), with similar gains on a mixed adult-pediatric dataset (94.67% vs 94.17%), suggesting improved artifact resistance through anatomical alignment.
Significance. If the central assumption holds, the work shows that landmark-driven geometric normalization can yield more controlled representations for CXR classification that are less influenced by acquisition artifacts and shape variation, with empirical support from public datasets and cross-validation that includes pediatric cases. This could inform future efforts in standardizing anatomical alignment for pulmonary disease detection.
major comments (1)
- [Abstract / geometric normalizer description] The central claim that normalized images provide a more artifact-resistant representation rests on the premise that 15 contour landmarks (mean error 3.61 pixels) plus piecewise affine warping preserve disease-relevant internal features such as opacities and consolidations. No quantitative check (e.g., sensitivity analysis on landmark error or pre/post-warping texture/feature comparison) is reported to substantiate that the residual localization error leaves these signals unchanged.
minor comments (1)
- [Results] Accuracy differences are given with 5-fold CV standard deviations but without statistical significance testing (e.g., paired tests on the per-fold results) to establish whether the reported gains over masked/cropped baselines are reliable.
Simulated Author's Rebuttal
We thank the referee for the constructive comment on our manuscript. We address the major point below and will strengthen the validation of feature preservation in the revision.
read point-by-point responses
-
Referee: [Abstract / geometric normalizer description] The central claim that normalized images provide a more artifact-resistant representation rests on the premise that 15 contour landmarks (mean error 3.61 pixels) plus piecewise affine warping preserve disease-relevant internal features such as opacities and consolidations. No quantitative check (e.g., sensitivity analysis on landmark error or pre/post-warping texture/feature comparison) is reported to substantiate that the residual localization error leaves these signals unchanged.
Authors: We agree that a direct quantitative check on internal feature preservation would strengthen the central claim. The manuscript currently provides indirect support via classification gains over artifact-masked baselines and Grad-CAM visualizations, but does not include sensitivity analysis on landmark error or pre/post-warping texture comparisons. In the revised manuscript we will add: (1) a sensitivity study perturbing the 15 landmarks within the observed 3.61-pixel mean error and measuring impact on classifier logits and Grad-CAM heatmaps; (2) quantitative texture/feature comparisons (e.g., local entropy, contrast, and Haralick features) computed on disease-relevant regions before and after warping. These additions will be reported in a new subsection of the experiments. revision: yes
Circularity Check
No significant circularity; empirical comparisons are independent of inputs
full rationale
The paper reports measured landmark localization error (3.61 px) from a ResNet-18 ensemble, applies standard GPA + Delaunay + piecewise affine warping, and evaluates classification accuracy on held-out public datasets via five-fold cross-validation. The central result (normalized images outperforming masked/cropped baselines at 98.60% vs 96.24% and 94.67% vs 94.17%) is a direct empirical comparison with no reduction of any claimed prediction to a fitted parameter, self-definition, or self-citation chain. All steps remain falsifiable against external data and do not collapse by construction.
Axiom & Free-Parameter Ledger
free parameters (1)
- Number of landmarks
axioms (1)
- domain assumption A set of 15 landmarks on the lung contour is sufficient to represent shape variation for the purpose of piecewise affine normalization.
Reference graph
Works this paper leans on
-
[1]
Use of Chest Imaging in COVID-19: A Rapid Advice Guide
World Health Organization. Use of Chest Imaging in COVID-19: A Rapid Advice Guide. Technical report, World Health Organization, Geneva, Switzerland, 2020
2020
-
[2]
CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning
Pranav Rajpurkar, Jeremy Irvin, Kaylie Zhu, Brandon Yang, Hershel Mehta, Tony Duan, Daisy Ding, Aarti Bagul, Curtis Langlotz, Katie Shpanskaya, et al. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning.arXiv preprint arXiv:1711.05225, 2017
work page internal anchor Pith review Pith/arXiv arXiv 2017
-
[3]
COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images.Scientific Reports, 10:19549, 2020
Linda Wang, Zhong Qiu Lin, and Alexander Wong. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images.Scientific Reports, 10:19549, 2020
2020
-
[4]
Muhammad E. H. Chowdhury, Tawsifur Rahman, Amith Khandakar, Rashid Mazhar, Muhammad A. Kadir, Zaid Bin Mahbub, Khandaker R. Islam, Muhammad Salman Khan, Atif Iqbal, Nasser Al Emadi, et al. Can AI Help in Screening Viral and COVID-19 Pneumonia?IEEE Access, 8:132665–132676, 2020
2020
-
[5]
Zech, Marcus A
John R. Zech, Marcus A. Badgeley, Manway Liu, Anthony B. Costa, Joseph J. Titano, and Eric Karl Oermann. Variable generalization performance of a deep learning model to detect pneumonia in chest radiographs: A cross-sectional study.PLoS Medicine, 15:e1002683, 2018
2018
-
[6]
Ayala-Raggi, Alejandro E
Salvador E. Ayala-Raggi, Alejandro E. Picazo-Castillo, Aldrin Barreto-Flores, and José F. Portillo-Robledo. Synergizing chest X-ray image normalization and discriminative feature selection for efficient and automatic COVID-19 recognition. InPattern Recognition. ACPR 2023, volume 14407 ofLecture Notes in Computer Science, pages 224–238, Cham, Switzerland, ...
2023
-
[7]
Picazo-Castillo, Salvador E
Alejandro E. Picazo-Castillo, Salvador E. Ayala-Raggi, Luis Altamirano-Robles, Aldrin Barreto-Flores, and José F. Portillo- Robledo. Comparative study of lung image representations for automated pneumonia recognition.International Journal of Combinatorial Optimization Problems and Informatics, 15:193–201, 2024
2024
-
[8]
Spatial transformer networks
Max Jaderberg, Karen Simonyan, Andrew Zisserman, and Koray Kavukcuoglu. Spatial transformer networks. InAdvances in Neural Information Processing Systems, volume 28, pages 2017–2025, 2015
2017
-
[9]
John C. Gower. Generalized Procrustes analysis.Psychometrika, 40:33–51, 1975
1975
-
[10]
Sur la sphère vide.Izvestia Akademii Nauk SSSR, 7:793–800, 1934
Boris Delaunay. Sur la sphère vide.Izvestia Akademii Nauk SSSR, 7:793–800, 1934
1934
-
[11]
IEEE Computer Society Press, Los Alamitos, CA, USA, 1990
George Wolberg.Digital Image Warping. IEEE Computer Society Press, Los Alamitos, CA, USA, 1990
1990
-
[12]
Deep residual learning for image recognition
Kaiming He, Xiangyu Zhang, Shaoqing Ren, and Jian Sun. Deep residual learning for image recognition. InProceedings of the IEEE Conference on Computer Vision and Pattern Recognition, pages 770–778, Las Vegas, NV , USA, 2016
2016
-
[13]
Tariqul Islam, Somaya Al Maadeed, Susu M
Tawsifur Rahman, Amith Khandakar, Yazan Qiblawey, Anas Tahir, Serkan Kiranyaz, Saad Bin Abul Kashem, Md. Tariqul Islam, Somaya Al Maadeed, Susu M. Zughaier, Muhammad Salman Khan, et al. Exploring the effect of image enhancement techniques on COVID-19 detection using chest X-ray images.Computers in Biology and Medicine, 132:104319, 2021
2021
-
[14]
ImageNet: A large-scale hierarchical image database
Jia Deng, Wei Dong, Richard Socher, Li-Jia Li, Kai Li, and Li Fei-Fei. ImageNet: A large-scale hierarchical image database. InProceedings of the IEEE Conference on Computer Vision and Pattern Recognition, pages 248–255, Miami, FL, USA, 2009
2009
-
[15]
Coordinate attention for efficient mobile network design
Qibin Hou, Daquan Zhou, and Jiashi Feng. Coordinate attention for efficient mobile network design. InProceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, pages 13713–13722, Nashville, TN, USA, 2021
2021
-
[16]
Group normalization
Yuxin Wu and Kaiming He. Group normalization. InProceedings of the European Conference on Computer Vision, pages 3–19, Munich, Germany, 2018
2018
-
[17]
Wing loss for robust facial landmark localisation with convolutional neural networks
Zhen-Hua Feng, Josef Kittler, Muhammad Awais, Patrik Huber, and Xiao-Jun Wu. Wing loss for robust facial landmark localisation with convolutional neural networks. InProceedings of the IEEE Conference on Computer Vision and Pattern Recognition, pages 2235–2245, Salt Lake City, UT, USA, 2018
2018
-
[18]
Rafael A. Cruz Ovando, Salvador E. Ayala Raggi, Alejandro E. Picazo Castillo, and Aldrin Barreto Flores. Statistical Asymmetrical Histogram Stretching for Contrast Enhancement in Chest X-ray Images for Pneumonia Detection.Computación y Sistemas, 29(4), 2025. doi:10.13053/cys-29-4-6115
-
[19]
Decoupled weight decay regularization
Ilya Loshchilov and Frank Hutter. Decoupled weight decay regularization. InProceedings of the International Conference on Learning Representations, New Orleans, LA, USA, 2019. 16 This manuscript is currently under consideration for publication.ARXIVPREPRINT
2019
-
[20]
Cell172(5), 1122– 1131.e9 (2018).https://doi.org/10.1016/j.cell.2018.02.010
Daniel S. Kermany, Michael Goldbaum, Wenjia Cai, Carolina C. S. Valentim, Huiying Liang, Sally L. Baxter, Alex McKeown, Ge Yang, Xiaokang Wu, Fangbing Yan, et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning.Cell, 172(5):1122–1131, 2018. doi:10.1016/j.cell.2018.02.010
-
[21]
Rajendra Acharya
Tulin Özturk, Muhammed Talo, Eylul Azra Yildirim, Ulas Baran Baloglu, Ozal Yildirim, and U. Rajendra Acharya. Automated detection of COVID-19 cases using deep neural networks with X-ray images.Computers in Biology and Medicine, 121:103792, 2020
2020
-
[22]
Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks.Pattern Analysis and Applications, 24:1207–1220, 2021
Ali Narin, Ceren Kaya, and Ziynet Pamuk. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks.Pattern Analysis and Applications, 24:1207–1220, 2021. 17
2021
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.