Region-Grounded Report Generation for 3D Medical Imaging: A Fine-Grained Dataset and Graph-Enhanced Framework
Pith reviewed 2026-05-19 18:08 UTC · model grok-4.3
The pith
Graph-based framework with region annotations generates more reliable reports from 3D PET/CT scans.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
By grounding report generation in fine-grained RoI annotations and using graph-based relational modules to capture dependencies between RoI attributes, the framework shifts from whole-volume mapping to localized clinical reasoning, achieving state-of-the-art results with gains of 19.7% in BLEU, 4.7% in ROUGE-L, and 45.8% in new clinical metrics that quantify RoI coverage and description quality.
What carries the argument
Graph-based relational modules that capture dependencies between RoI attributes, enabling the model to mimic radiologist analysis of localized findings instead of global volume patterns.
If this is right
- Reports exhibit greater fidelity to specific localized findings, lowering the rate of unsupported statements.
- The introduced RoI Coverage and RoI Quality Index metrics offer a more targeted way to assess clinical reliability beyond text overlap scores.
- Performance gains indicate the method can support report generation in data-scarce settings for languages with limited medical corpora.
- The dataset enables training and benchmarking of future models that explicitly reason over annotated regions.
Where Pith is reading between the lines
- The same graph approach could be tested on other 3D modalities such as MRI to check whether RoI grounding transfers without new manual annotations.
- Pairing the framework with automated RoI detectors might remove the need for human-provided region labels at inference time.
- Extending the clinical metrics to measure consistency across multiple radiologist reports could further validate reduced hallucination.
Load-bearing premise
The assumption that graph-based relational modules accurately capture clinically meaningful dependencies between RoI attributes and that LLM-based extraction for RoI Coverage and RoI Quality Index provides an unbiased measure of report fidelity.
What would settle it
If disabling the graph relational modules in HiRRA produces no measurable drop in RoI Coverage and RoI Quality Index scores on the held-out test set, the claimed benefit of modeling attribute dependencies would not hold.
Figures




read the original abstract
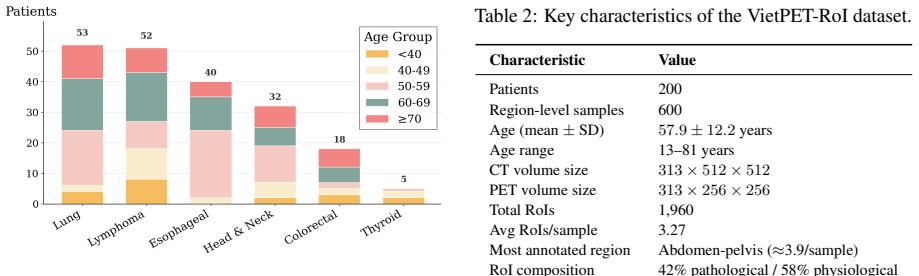
Automated medical report generation for 3D PET/CT imaging is fundamentally challenged by the high-dimensional nature of volumetric data and a critical scarcity of annotated datasets, particularly for low-resource languages. Current black-box methods map whole volumes to reports, ignoring the clinical workflow of analyzing localized Regions of Interest (RoIs) to derive diagnostic conclusions. In this paper, we bridge this gap by introducing VietPET-RoI, the first large-scale 3D PET/CT dataset with fine-grained RoI annotation for a low-resource language, comprising 600 PET/CT samples and 1,960 manually annotated RoIs, paired with corresponding clinical reports. Furthermore, to demonstrate the utility of this dataset, we propose HiRRA, a novel framework that mimics the professional radiologist diagnostic workflow by employing graph-based relational modules to capture dependencies between RoI attributes. This approach shifts from global pattern matching toward localized clinical findings. Additionally, we introduce new clinical evaluation metrics, namely RoI Coverage and RoI Quality Index, that measure both RoI localization accuracy and attribute description fidelity using LLM-based extraction. Extensive evaluation demonstrates that our framework achieves SOTA performance, surpassing existing models by 19.7% in BLEU and 4.7% in ROUGE-L, while achieving a remarkable 45.8% improvement in clinical metrics, indicating enhanced clinical reliability and reduced hallucination. Our code and dataset are available on GitHub.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces VietPET-RoI, the first large-scale 3D PET/CT dataset with fine-grained RoI annotations (600 samples, 1,960 RoIs) paired with clinical reports in a low-resource language. It proposes the HiRRA framework, which uses graph-based relational modules to model dependencies between RoI attributes in a manner that mimics radiologist diagnostic workflow. New clinical metrics (RoI Coverage and RoI Quality Index) are defined via LLM-based extraction of attributes from generated reports. The work claims state-of-the-art results with gains of 19.7% in BLEU, 4.7% in ROUGE-L, and 45.8% in the new clinical metrics, along with reduced hallucination.
Significance. If validated, the dataset would address a clear gap in annotated 3D medical imaging data for low-resource languages, and the region-grounded graph approach could shift the field away from whole-volume black-box methods. The new clinical metrics offer a potential way to quantify localization and fidelity beyond standard NLG scores. Releasing code and data supports reproducibility, which is a strength.
major comments (3)
- [Evaluation section] Evaluation section: The 45.8% improvement in clinical metrics (RoI Coverage and RoI Quality Index) is defined via LLM-based attribute extraction and comparison to ground-truth RoIs, yet no validation of the LLM extractor (e.g., agreement with radiologists, precision/recall on attribute extraction, or error analysis) is reported. This is load-bearing for the claim of enhanced clinical reliability and reduced hallucination.
- [Framework section] Framework section: The graph-based relational modules are asserted to capture clinically meaningful dependencies between RoI attributes, but no independent check (such as expert review of learned relations or targeted ablation isolating their contribution to the reported gains) is provided.
- [Experimental Setup] Experimental Setup: Full details on data splits, complete ablation studies, and error analysis are absent, preventing independent verification of the SOTA claims on BLEU, ROUGE-L, and clinical metrics.
minor comments (1)
- [Abstract] Abstract: The language of the reports is described only as 'low-resource' without naming it explicitly.
Simulated Author's Rebuttal
We thank the referee for their thorough review and constructive comments. We address each of the major comments below, indicating the changes we will make to the manuscript.
read point-by-point responses
-
Referee: [Evaluation section] The 45.8% improvement in clinical metrics (RoI Coverage and RoI Quality Index) is defined via LLM-based attribute extraction and comparison to ground-truth RoIs, yet no validation of the LLM extractor (e.g., agreement with radiologists, precision/recall on attribute extraction, or error analysis) is reported. This is load-bearing for the claim of enhanced clinical reliability and reduced hallucination.
Authors: We agree that validating the LLM extractor is important for substantiating the clinical metrics. In the revised manuscript, we will add a validation subsection where we report inter-rater agreement between the LLM extractor and radiologist annotations on a sample of reports, along with precision and recall for attribute extraction. This will support the claims of reduced hallucination and enhanced reliability. revision: yes
-
Referee: [Framework section] The graph-based relational modules are asserted to capture clinically meaningful dependencies between RoI attributes, but no independent check (such as expert review of learned relations or targeted ablation isolating their contribution to the reported gains) is provided.
Authors: We will enhance the framework section with a targeted ablation study that isolates the impact of the graph-based relational modules on the performance gains. Additionally, we will include qualitative examples or analysis of the learned relations to demonstrate their clinical relevance. revision: yes
-
Referee: [Experimental Setup] Full details on data splits, complete ablation studies, and error analysis are absent, preventing independent verification of the SOTA claims on BLEU, ROUGE-L, and clinical metrics.
Authors: We acknowledge the need for more comprehensive experimental details. In the revision, we will include explicit descriptions of the data splits (including ratios and stratification criteria), present complete ablation studies for all components, and add an error analysis section discussing common failure modes and how the proposed method addresses them. revision: yes
Circularity Check
No significant circularity in derivation or evaluation chain
full rationale
The paper introduces an external dataset (VietPET-RoI) and a new framework (HiRRA) whose graph modules are motivated by clinical workflow description rather than by the target metrics. Reported gains are measured on standard external benchmarks (BLEU, ROUGE-L) plus newly defined clinical scores; these scores are computed from LLM extraction applied after generation and are not used as training objectives or fitted parameters. No equations, self-citations, or ansatzes are shown to reduce the claimed improvements to quantities defined inside the paper itself. The evaluation therefore remains an independent empirical comparison against prior models.
Axiom & Free-Parameter Ledger
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/AlexanderDuality.leanalexander_duality_circle_linking unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
HiRRA... employs graph-based relational modules to capture dependencies between RoI attributes... GATv2... edges based on spatial proximity and morphological similarity
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
new clinical evaluation metrics, namely RoI Coverage and RoI Quality Index, that measure both RoI localization accuracy and attribute description fidelity using LLM-based extraction
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Roi-based compression strategy of 3d mri brain datasets for wireless communications.IRBM, 42(3):146–153. Sergios Gatidis, Tobias Hepp, Marcel Früh, Christian La Fougère, Konstantin Nikolaou, Christina Pfannen- berg, Bernhard Schölkopf, Thomas Küstner, Clemens Cyran, and Daniel Rubin. 2022. A whole-body fdg- pet/ct dataset with manually annotated tumor les...
-
[2]
Med3dvlm: An efficient vision–language model for 3d medical image analysis.IEEE Journal of Biomedical and Health Informatics. To appear. Junsan Zhang, Ming Cheng, Qiaoqiao Cheng, Xiuxuan Shen, Yao Wan, Jie Zhu, and Mengxuan Liu. 2024. Hierarchical medical image report adversarial genera- tion with hybrid discriminator.Artificial Intelligence in Medicine, ...
-
[3]
- [Very intense focal FDG uptake (SUVmax 12.3) in the cecum. Highly suggestive of colon cancer...] B.2 Information Extraction Framework To evaluate generation quality, we employLangEx- tract(Goel, 2025), an LLM-based extraction frame- work designed to parse unstructured generated re- ports into structured RoI objects. Specifically, we utilize Gemini-2.5-P...
work page 2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.