Clinical Assistant for Remote Engagement Link (CARE-link): A Web-Based Electronic Health Records Software for Managing Diabetes
Pith reviewed 2026-06-28 04:16 UTC · model grok-4.3
The pith
CARE-link is a web-based platform that uses an LLM to link clinicians and patients for continuous gestational diabetes management.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
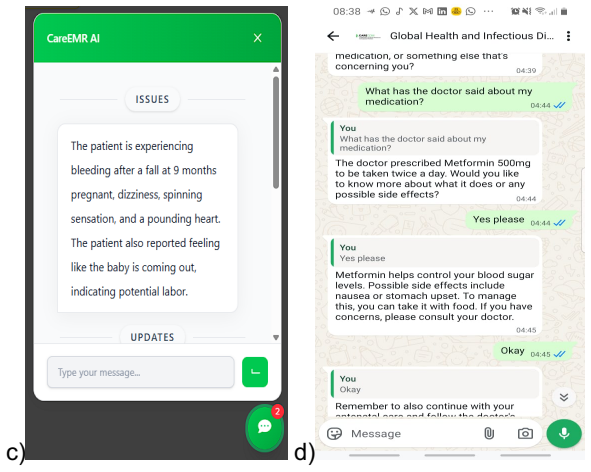
CARE-link is an open-source, web-based clinical support platform designed to improve the management of gestational diabetes by linking clinicians and patients through an LLM-mediated workflow. The system aggregates patient-generated data outside the hospital, summarizes relevant clinical information, and delivers context-aware decision support to clinicians. For patients, CARE-link provides clear explanations of management plans and delivers timely lifestyle guidance through a WhatsApp interface. The integrated dual-facing design aims to promote continuous monitoring, support individualized care, and reduce the burden of in-clinic follow-ups. Built with a modular architecture, the platform c
What carries the argument
The LLM-mediated dual-facing workflow that aggregates patient data, summarizes it for clinicians, and delivers guidance to patients via WhatsApp.
If this is right
- Continuous remote monitoring of gestational diabetes becomes feasible without daily clinic contact.
- Patient compliance can increase through timely, personalized WhatsApp messages.
- In-clinic follow-up visits decrease while clinical oversight stays intact.
- The modular design allows the same platform to handle other chronic conditions that need ongoing tracking.
- Resource-constrained clinics gain a tool to strengthen continuity of care at lower operational cost.
Where Pith is reading between the lines
- Similar LLM-mediated interfaces could be tested for hypertension or type 2 diabetes management where behavioral support matters.
- Integration with existing hospital electronic records systems would be a next practical step to check data flow.
- Measuring actual reduction in clinic visits and changes in patient HbA1c or compliance rates would provide direct evidence of impact.
Load-bearing premise
That the LLM can reliably aggregate patient data, summarize clinical information, and give accurate guidance without introducing errors that would require extensive human checking.
What would settle it
A controlled test in which clinicians review LLM-generated summaries and patient guidance from CARE-link and find a measurable rate of factual errors or unsafe recommendations that change care decisions.
Figures

read the original abstract
CARE-link is an open-source, web-based clinical support platform designed to improve the management of gestational diabetes by linking clinicians and patients through an LLM-mediated workflow. The system aggregates patient-generated data outside the hospital, summarizes relevant clinical information, and delivers context-aware decision support to clinicians. For patients, CARE-link provides clear explanations of management plans and delivers timely lifestyle guidance through a WhatsApp interface. The integrated dual-facing design aims to promote continuous monitoring, support individualized care, and reduce the burden of in-clinic follow-ups. Built with a modular architecture, the platform can be adapted to other chronic conditions requiring longitudinal tracking and behavioral support. CARE-link has the potential to enhance clinical oversight, promote patient compliance, and strengthen continuity of care particularly in resource-constrained settings.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents CARE-link, an open-source web-based electronic health records software for managing gestational diabetes. It describes a dual-facing LLM-mediated workflow that aggregates patient-generated data, summarizes clinical information for clinicians, and provides explanations and lifestyle guidance to patients via WhatsApp. The system aims to promote continuous monitoring, individualized care, and reduce in-clinic follow-ups, with a modular architecture adaptable to other chronic conditions.
Significance. If the described workflow performs reliably, the platform could improve continuity of care and reduce follow-up burden in resource-constrained settings. The open-source release and modular architecture are explicit strengths that could support adaptation and community use. The absence of any validation data, however, means these benefits remain hypothetical.
major comments (2)
- [Abstract] Abstract: The claims that the dual-facing LLM workflow 'aims to promote continuous monitoring, support individualized care' and 'has the potential to enhance clinical oversight, promote patient compliance' rest on the premise that the model aggregates data and issues guidance without clinically significant errors; the manuscript contains no accuracy metrics, hallucination audits, clinician review results, or safety thresholds for these LLM components.
- [System Architecture] The description of the LLM-mediated workflow for context-aware decision support and lifestyle guidance provides no discussion of error-handling protocols, human oversight requirements, or failure modes, which directly underpins the central assertion of strengthened continuity of care.
minor comments (2)
- The title refers to 'Managing Diabetes' while the abstract and claims focus on gestational diabetes; clarify the intended scope.
- A related-work section would help situate the modular LLM integration against existing telehealth and chronic-disease management platforms.
Simulated Author's Rebuttal
We thank the referee for their constructive comments on the CARE-link manuscript. We address each major comment below and agree that revisions are needed to clarify the scope of the claims and to address safety considerations.
read point-by-point responses
-
Referee: [Abstract] Abstract: The claims that the dual-facing LLM workflow 'aims to promote continuous monitoring, support individualized care' and 'has the potential to enhance clinical oversight, promote patient compliance' rest on the premise that the model aggregates data and issues guidance without clinically significant errors; the manuscript contains no accuracy metrics, hallucination audits, clinician review results, or safety thresholds for these LLM components.
Authors: We agree that the abstract uses forward-looking language about the intended benefits of the LLM workflow. This manuscript is a system description paper rather than an empirical evaluation, so no validation metrics are included. In revision we will rephrase the abstract to state that these outcomes are design goals and potential benefits, with explicit mention that empirical validation of the LLM components is planned for future work. revision: yes
-
Referee: [System Architecture] The description of the LLM-mediated workflow for context-aware decision support and lifestyle guidance provides no discussion of error-handling protocols, human oversight requirements, or failure modes, which directly underpins the central assertion of strengthened continuity of care.
Authors: The referee is correct that the current architecture section omits discussion of safety mechanisms. We will add a new subsection on safety and oversight that describes the requirement for clinician review of all LLM outputs, basic error-handling (e.g., fallback to standard messaging), and known failure modes such as hallucination or context loss. This addition will be placed under System Architecture and will also reference planned future safety audits. revision: yes
Circularity Check
No circularity: system-description paper with no derivations or fitted predictions
full rationale
The manuscript is a high-level description of a web-based EHR platform using LLM-mediated workflows for gestational diabetes management. It contains no equations, no parameter fitting, no predictions derived from inputs, and no self-citation chains that bear the central claims. The dual-facing design and potential benefits are presented as design goals and aspirational outcomes rather than results obtained by reducing one quantity to another by construction. The reader's assessment of circularity score 0.0 is confirmed; the paper is self-contained as an engineering/systems contribution without internal reasoning loops that collapse to their own inputs.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
1 Clinical Assistant for Remote Engagement Link (CARE-link): A Web-Based Electronic Health Records Software for Managing Diabetes *Adjei Prince Ebenezera,b,c, Tettey Teye Joshuaa,b, Musah Toufiqb, Agbeve Audreya,b, John Amuasia,b,d aGlobal One Health Research Group, Bernhard Nocht Institute of Tropical Medicine, Bernhard-Nocht-Str. 74, 20359 Hamburg, Germ...
1936
-
[2]
S. Kitsiou, G. Paré, M. Jaana, and B. Gerber, “Effectiveness of mHealth interventions for patients with diabetes: An overview of systematic reviews,” PLOS ONE, vol. 12, no. 3, p. e0173160, Mar. 2017, doi: 10.1371/journal.pone.0173160
-
[3]
R. Tarricone, F. Petracca, L. Svae, M. Cucciniello, and O. Ciani, “Which behaviour change techniques work best for diabetes self-management mobile apps? Results from a systematic review and meta-analysis of randomised controlled trials,” eBioMedicine, vol. 103, p. 105091, May 2024, doi: 10.1016/j.ebiom.2024.105091
-
[4]
O. Olakotan, R. Samuriwo, H. Ismaila, and S. Atiku, “Usability Challenges in Electronic Health Records: Impact on Documentation Burden and Clinical Workflow: A Scoping Review,” J. Eval. Clin. Pract., vol. 31, no. 4, p. e70189, June 2025, doi: 10.1111/jep.70189
-
[5]
A. Mwogosi, D. Shao, S. Kibusi, and N. Kapologwe, “Revolutionizing decision support: a systematic literature review of contextual implementation models for electronic health 10 records systems,” J. Health Organ. Manag., vol. 38, no. 3, pp. 372–388, May 2024, doi: 10.1108/JHOM-04-2023-0122
-
[6]
Prospects for AI clinical summarization to reduce the burden of patient chart review,
C. Lee, K. A. Vogt, and S. Kumar, “Prospects for AI clinical summarization to reduce the burden of patient chart review,” Front. Digit. Health, vol. 6, p. 1475092, Nov. 2024, doi: 10.3389/fdgth.2024.1475092
-
[8]
K. S. Safo, D. Opoku, R. A. Bonney, C. K. Serchim, and K. A. Mensah, “Potential effects of Whatsapp on maternal health services uptake during COVID-19: a cross-sectional study in Ghana,” BMC Health Serv. Res., vol. 25, no. 1, p. 72, Jan. 2025, doi: 10.1186/s12913-025-12245-3
-
[9]
Using WhatsApp messenger for health systems research: a scoping review of available literature,
K. Manji, J. Hanefeld, J. Vearey, H. Walls, and T. De Gruchy, “Using WhatsApp messenger for health systems research: a scoping review of available literature,” Health Policy Plan., vol. 36, no. 5, pp. 774–789, June 2021, doi: 10.1093/heapol/czab024
-
[10]
Y. Chen, C. U. Lehmann, and B. Malin, “Digital Information Ecosystems in Modern Care Coordination and Patient Care Pathways and the Challenges and Opportunities for AI Solutions,” J. Med. Internet Res., vol. 26, p. e60258, Dec. 2024, doi: 10.2196/60258
-
[11]
Evaluating clinical AI summaries with large language models as judges,
E. Croxford et al., “Evaluating clinical AI summaries with large language models as judges,” Npj Digit. Med., vol. 8, no. 1, p. 640, Nov. 2025, doi: 10.1038/s41746-025-02005-2
-
[12]
H. D. O. Campos, D. Wolfe, H. Luan, and I. Sim, “Generative AI as Third Agent: Large Language Models and the Transformation of the Clinician-Patient Relationship,” J. Particip. Med., vol. 17, pp. e68146–e68146, Aug. 2025, doi: 10.2196/68146
-
[13]
Artificial Intelligence–Generated Draft Replies to Patient Inbox Messages,
P. Garcia et al., “Artificial Intelligence–Generated Draft Replies to Patient Inbox Messages,” JAMA Netw. Open, vol. 7, no. 3, p. e243201, Mar. 2024, doi: 10.1001/jamanetworkopen.2024.3201
-
[14]
P. Khatiwada, B. Yang, J.-C. Lin, and B. Blobel, “Patient-Generated Health Data (PGHD): Understanding, Requirements, Challenges, and Existing Techniques for Data Security and Privacy,” J. Pers. Med., vol. 14, no. 3, p. 282, Mar. 2024, doi: 10.3390/jpm14030282
-
[15]
A. M. Jacome-Hortua, Z. R. Rincon-Rueda, D. C. Sanchez-Ramirez, and A. Angarita-Fonseca, “Effects of a WhatsApp-Assisted Health Educational Intervention for Cardiac Rehabilitation: A Randomized Controlled Clinical Trial Protocol,” Methods Protoc., vol. 7, no. 2, p. 35, Apr. 2024, doi: 10.3390/mps7020035
-
[16]
M. D. Owen et al., “Use of WhatsApp messaging technology to strengthen obstetric referrals in the Greater Accra Region, Ghana: Findings from a feasibility study,” PLOS ONE, vol. 17, no. 4, p. e0266932, Apr. 2022, doi: 10.1371/journal.pone.0266932
-
[17]
B. Ebenso, E. Namisango, I.-O. Abejirinde, and M. J. Allsop, “Editorial: The scale-up and sustainability of digital health interventions in low- and middle-income settings,” Front. Digit. Health, vol. 7, p. 1634223, Sept. 2025, doi: 10.3389/fdgth.2025.1634223
-
[18]
D. J. Cohen, S. R. Keller, G. R. Hayes, D. A. Dorr, J. S. Ash, and D. F. Sittig, “Integrating Patient-Generated Health Data Into Clinical Care Settings or Clinical Decision-Making: Lessons Learned From Project HealthDesign,” JMIR Hum. Factors, vol. 3, no. 2, p. e26, Oct. 2016, doi: 10.2196/humanfactors.5919
-
[19]
Washington, D.C.: National Academies Press, 2019, p
The Learning Health System Series and National Academy of Medicine, Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. Washington, D.C.: National Academies Press, 2019, p. 27111. doi: 10.17226/27111
-
[20]
Paying for artificial intelligence in medicine,
R. B. Parikh and L. A. Helmchen, “Paying for artificial intelligence in medicine,” Npj Digit. Med., vol. 5, no. 1, p. 63, May 2022, doi: 10.1038/s41746-022-00609-6. 11
-
[21]
Use of Ambient AI Scribes to Reduce Administrative Burden and Professional Burnout,
K. D. Olson et al., “Use of Ambient AI Scribes to Reduce Administrative Burden and Professional Burnout,” JAMA Netw. Open, vol. 8, no. 10, p. e2534976, Oct. 2025, doi: 10.1001/jamanetworkopen.2025.34976
-
[22]
Telehealth: Advances in Alternative Payment Models,
M. Zhao, H. Hamadi, D. R. Haley, J. Xu, C. White-Williams, and S. Park, “Telehealth: Advances in Alternative Payment Models,” Telemed. E-Health, vol. 26, no. 12, pp. 1492–1499, Dec. 2020, doi: 10.1089/tmj.2019.0294
-
[23]
Best practices in scaling digital health in low- and middle-income countries,
A. B. Labrique et al., “Best practices in scaling digital health in low- and middle-income countries,” Glob. Health, vol. 14, no. 1, p. 103, Dec. 2018, doi: 10.1186/s12992-018-0424-z
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.