Algorithms Trained on Normal Chest X-rays Can Predict Health Insurance Types
Pith reviewed 2026-05-17 22:30 UTC · model grok-4.3
The pith
Deep vision models predict a patient's health insurance type from normal chest X-rays at AUC around 0.70.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
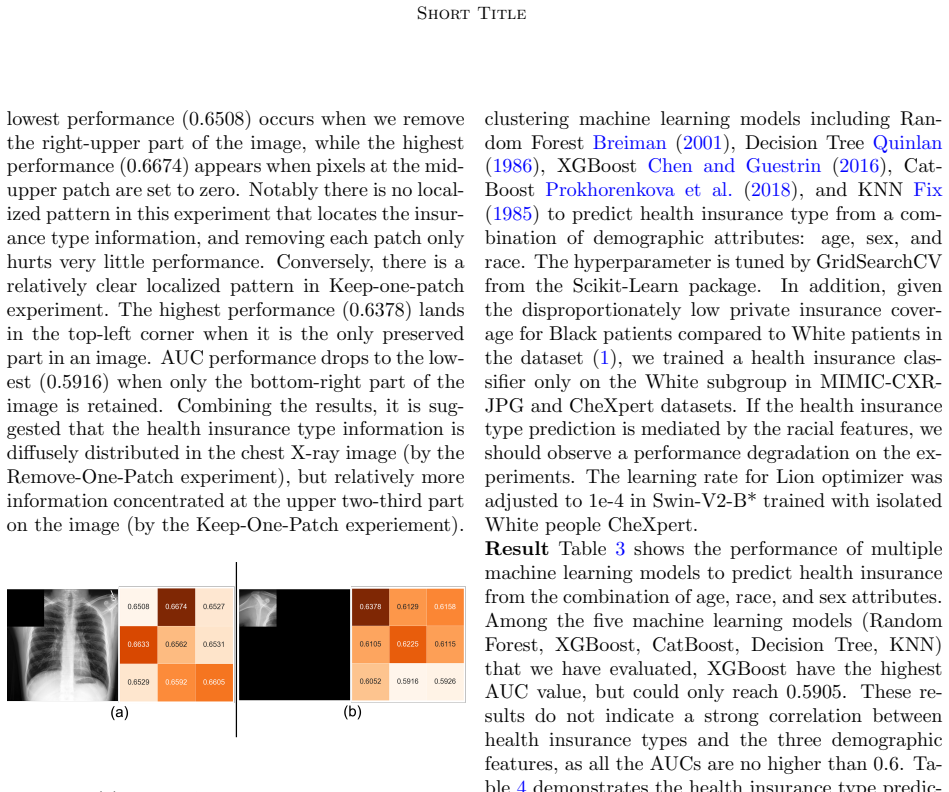
Deep vision models trained on chest X-rays from normal studies can predict a patient's health insurance type with AUC around 0.70 on MIMIC-CXR-JPG and 0.68 on CheXpert. The signal survives controls for demographic variables and remains detectable within a single racial group. Patch-based occlusion localizes the information diffusely in the upper and mid-thoracic regions, consistent with subtle differences in clinical environments, equipment, or care pathways that correlate with insurance status.
What carries the argument
Patch-based occlusion analysis that identifies a diffuse signal in the upper and mid-thoracic regions after demographic controls.
If this is right
- Medical images encode information about socioeconomic segregation through the pathways and hardware used to produce them.
- Fairness work in medical AI must examine data collection practices in addition to balancing patient demographics.
- Models may learn to associate insurance type with subtle imaging artifacts that arise from different care settings.
- Diagnostic algorithms could inadvertently use these hidden signals when deployed in real clinical workflows.
Where Pith is reading between the lines
- Audits of imaging hardware and site-specific protocols could reduce unintended socioeconomic leakage in future training sets.
- The same approach might reveal parallel signals in other imaging modalities such as CT or MRI.
- Developers could test whether explicit removal of hospital or scanner metadata during training eliminates the insurance prediction task.
Load-bearing premise
The models are picking up differences in clinical environments or equipment that happen to track insurance type rather than direct demographic features.
What would settle it
Retrain the same architectures on images acquired on identical equipment inside a single hospital for patients across all insurance types and check whether accuracy falls to chance level.
Figures
read the original abstract
Artificial intelligence is revealing what medicine never intended to encode. Deep vision models, trained on chest X-rays, can now detect not only disease but also invisible traces of social inequality. In this study, we show that state-of-the-art architectures (DenseNet121, SwinV2-B, MedMamba) can predict a patient's health insurance type, a strong proxy for socioeconomic status, from normal chest X-rays with significant accuracy (AUC around 0.70 on MIMIC-CXR-JPG, 0.68 on CheXpert). The signal was unlikely contributed by demographic features by our machine learning study combining age, race, and sex labels to predict health insurance types; it also remains detectable when the model is trained exclusively on a single racial group. Patch-based occlusion reveals that the signal is diffuse rather than localized, embedded in the upper and mid-thoracic regions. This suggests that deep networks may be internalizing subtle traces of clinical environments, equipment differences, or care pathways; learning socioeconomic segregation itself. These findings challenge the assumption that medical images are neutral biological data. By uncovering how models perceive and exploit these hidden social signatures, this work reframes fairness in medical AI: the goal is no longer only to balance datasets or adjust thresholds, but to interrogate and disentangle the social fingerprints embedded in clinical data itself.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents empirical evidence that deep neural networks (DenseNet121, SwinV2-B, MedMamba) trained on 'normal' chest X-rays from the MIMIC-CXR-JPG and CheXpert datasets can predict a patient's health insurance type—a proxy for socioeconomic status—with AUCs of approximately 0.70 and 0.68, respectively. The authors argue that this predictive capability is not primarily attributable to demographic variables (age, race, sex) based on auxiliary prediction experiments and single-race subgroup training, and interpret patch-based occlusion maps as indicating a diffuse signal in the upper and mid-thoracic regions, potentially reflecting clinical environment or care pathway differences.
Significance. If the central empirical result holds after addressing institutional confounders, the work would be significant for medical AI fairness research by showing that routine chest X-rays can encode socioeconomic information via subtle institutional cues. Credit is due for evaluating multiple modern architectures on public datasets and including occlusion-based interpretability analysis, which provides a concrete starting point for reproducibility.
major comments (3)
- [Abstract] Abstract: The assertion that the signal 'was unlikely contributed by demographic features' rests on an auxiliary 'machine learning study combining age, race, and sex labels' whose quantitative results (e.g., AUC of the demographic-only predictor versus the imaging model) are not reported, preventing evaluation of whether demographics are adequately controlled.
- [Abstract] Abstract: Both MIMIC-CXR-JPG and CheXpert are single-institution datasets; the manuscript does not control for or discuss confounding by acquisition device, department, or workflow factors that correlate with insurance type. The reported demographic controls and single-race subgroup results do not address these institutional variables, which remain a load-bearing alternative explanation for the observed AUCs.
- [Abstract] Abstract: No information is provided on train/test splits, class balance for insurance categories, preprocessing steps, or statistical testing (confidence intervals, p-values) for the reported AUCs of 0.70 and 0.68, limiting assessment of result robustness.
minor comments (2)
- [Abstract] The abstract uses 'significant accuracy' without accompanying statistical tests or effect-size context; replace with precise quantitative language.
- Consider adding explicit discussion of dataset limitations and generalizability in a dedicated limitations paragraph.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed comments. We have revised the abstract and expanded the discussion to address the concerns about transparency, controls, and methodological details.
read point-by-point responses
-
Referee: [Abstract] Abstract: The assertion that the signal 'was unlikely contributed by demographic features' rests on an auxiliary 'machine learning study combining age, race, and sex labels' whose quantitative results (e.g., AUC of the demographic-only predictor versus the imaging model) are not reported, preventing evaluation of whether demographics are adequately controlled.
Authors: We agree that the abstract should report the quantitative results of the auxiliary demographic study for proper evaluation. The full manuscript describes this control experiment; we have revised the abstract to explicitly summarize that the combined demographic model (age, race, sex) shows lower performance than the imaging model, with the specific AUC values and methodology now highlighted in the abstract and cross-referenced to the main text. revision: yes
-
Referee: [Abstract] Abstract: Both MIMIC-CXR-JPG and CheXpert are single-institution datasets; the manuscript does not control for or discuss confounding by acquisition device, department, or workflow factors that correlate with insurance type. The reported demographic controls and single-race subgroup results do not address these institutional variables, which remain a load-bearing alternative explanation for the observed AUCs.
Authors: We acknowledge this as a substantive concern. The manuscript already interprets the diffuse signal as potentially arising from clinical environment or care pathway differences, which are institutional. However, the single-race subgroup analysis controls for race but does not isolate device or workflow factors. In the revision we have added an explicit limitations paragraph in the Discussion acknowledging these institutional confounders as a plausible alternative and recommending multi-institutional validation in future work. revision: yes
-
Referee: [Abstract] Abstract: No information is provided on train/test splits, class balance for insurance categories, preprocessing steps, or statistical testing (confidence intervals, p-values) for the reported AUCs of 0.70 and 0.68, limiting assessment of result robustness.
Authors: We thank the referee for noting this omission in the abstract. These details appear in the Methods section of the full manuscript. We have revised the abstract to concisely include the patient-level train/test split approach, insurance category distributions, standard preprocessing steps, and the bootstrap procedure used to obtain confidence intervals around the reported AUCs. revision: yes
Circularity Check
Empirical ML evaluation on held-out data with no self-referential derivations
full rationale
The paper reports AUC performance from training standard vision architectures on public datasets (MIMIC-CXR-JPG, CheXpert) and evaluating on held-out test splits. No equations, ansatzes, or derivations are presented that would reduce the reported metrics to a parameter fitted directly to the insurance-type labels. Demographic controls and single-race subgroup experiments are additional empirical checks rather than definitional reductions. The central claim rests on observable model outputs against external test data and is therefore self-contained.
Axiom & Free-Parameter Ledger
free parameters (1)
- model training hyperparameters
axioms (1)
- domain assumption Normal chest X-rays contain diffuse visual features correlated with socioeconomic status via clinical environment or equipment differences
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
state-of-the-art architectures (DenseNet121, SwinV2-B, MedMamba) can predict a patient's health insurance type... AUC around 0.70 on MIMIC-CXR-JPG, 0.68 on CheXpert
-
IndisputableMonolith/Foundation/AlexanderDuality.leanalexander_duality_circle_linking unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
Patch-based occlusion reveals that the signal is diffuse rather than localized, embedded in the upper and mid-thoracic regions
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Forward citations
Cited by 1 Pith paper
-
Quantum Kernel Advantage over Classical Collapse in Medical Foundation Model Embeddings
Quantum kernels in QSVM deliver higher minority-class F1 scores than classical linear or RBF kernels on medical foundation model embeddings for binary insurance classification, avoiding classical collapse in noiseless...
Reference graph
Works this paper leans on
-
[1]
Pierre Chambon, Jean-Benoit Delbrouck, Thomas Sounack, Shih-Cheng Huang, Zhihong Chen, Maya 7 Short Title Varma, Steven QH Truong, Chu The Chuong, and Curtis P Langlotz. Chexpert plus: Augmenting a large chest x-ray dataset with text radiology re- ports, patient demographics and additional image formats.arXiv preprint arXiv:2405.19538,
-
[2]
MIMIC-CXR-JPG, a large publicly available database of labeled chest radiographs
Alistair Johnson, Matt Lungren, Yifan Peng, Zhiy- ong Lu, Roger Mark, Seth Berkowitz, and Steven Horng. Mimic-cxr-jpg-chest radiographs with structured labels.PhysioNet, 101:215–220, 2019a. Alistair EW Johnson, Tom J Pollard, Nathaniel R Greenbaum, Matthew P Lungren, Chih-ying Deng, Yifan Peng, Zhiyong Lu, Roger G Mark, Seth J Berkowitz, and Steven Horng....
work page internal anchor Pith review Pith/arXiv arXiv 1901
-
[3]
Charaka Vinayak Kumar, Ashok Urlana, Gopichand Kanumolu, Bala Mallikarjunarao Garlapati, and Pruthwik Mishra. No llm is free from bias: A com- prehensive study of bias evaluation in large lan- guage models.arXiv preprint arXiv:2503.11985,
-
[4]
Cautious optimizers: Improving training with one line of code.arXiv preprint arXiv:2411.16085,
8 Short Title Kaizhao Liang, Lizhang Chen, Bo Liu, and Qiang Liu. Cautious optimizers: Improving training with one line of code.arXiv preprint arXiv:2411.16085,
-
[5]
Chexclusion: Fairness gaps in deep chest x-ray classifiers
Laleh Seyyed-Kalantari, Guanxiong Liu, Matthew McDermott, Irene Y Chen, and Marzyeh Ghas- semi. Chexclusion: Fairness gaps in deep chest x-ray classifiers. InBIOCOMPUTING 2021: pro- ceedings of the Pacific symposium, pages 232–243. World Scientific,
work page 2021
-
[6]
Medmamba: Vision mamba for medical image classification,
Yubiao Yue and Zhenzhang Li. Medmamba: Vi- sion mamba for medical image classification.arXiv preprint arXiv:2403.03849,
-
[7]
Dataset description MIMIC-IV v3.0 Johnson et al
Appendix A. Dataset description MIMIC-IV v3.0 Johnson et al. (2024,
work page 2024
-
[8]
is a large medical dataset containing over 265,000 pa- tients’ data collected at Beth Israel Deaconess Medi- cal Center in Boston, MA, in the intensive care unit or emergency department between 2008-2022, while MIMIC-CXR-JPG Johnson et al. (2019a,b) is an ex- tended image dataset for MIMIC-IV v3.0, including 377,110 chest X-ray images in total. On the oth...
work page 2008
-
[9]
The recent CheXpert Plus paper Chambon et al
The images were downsized to 390 x 320 in the downsized version. The recent CheXpert Plus paper Chambon et al. (2024) provides additional demographic infor- mation of each patient, including their health insur- ance type, race, sex, and age. 9
work page 2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.