Recognition: unknown
End-to-End Evaluation and Governance of an EHR-Embedded AI Agent for Clinicians
Pith reviewed 2026-05-07 10:26 UTC · model grok-4.3
The pith
A governance framework using clinician rubrics, live feedback, and controlled experiments makes continuous oversight of clinical AI agents achievable and effective.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
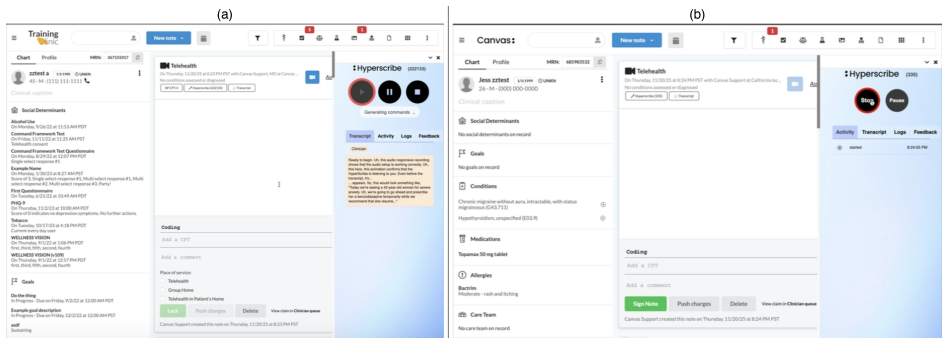
The authors demonstrate an integrated governance pipeline for an EHR-embedded agent that converts ambient audio into structured chart updates. Twenty clinicians authored 1,646 validated rubrics across 823 cases. Seven versions underwent controlled experiments that raised median quality scores from 84 percent to 95 percent. Analysis of 107 live feedback entries over three months showed error reports falling from 79 percent to 30 percent and positive observations rising to 45 percent as engineering fixes addressed issues. Median processing time per audio segment reached 8.1 seconds with a 99.6 percent effective completion rate after retry mechanisms handled transient errors. The work concludes
What carries the argument
The end-to-end governance framework that integrates rubric validation, live deployment feedback, technical performance monitoring, cost tracking, and controlled experimentation to gate system changes.
If this is right
- Quality scores for the AI agent rise systematically when governance data drives targeted engineering interventions.
- The share of positive feedback increases and error reports decrease as specific failures are identified and resolved over months of use.
- High completion rates and acceptable processing speeds can be sustained by adding retry logic for transient model errors.
- New versions of the agent can be tested in controlled experiments and blocked from full deployment if they do not meet rubric thresholds.
- Cost tracking alongside quality metrics supports decisions about whether to maintain or scale the deployed agent.
Where Pith is reading between the lines
- The same combination of rubrics and live feedback could be applied to other clinical AI tools such as diagnostic suggestion systems to keep their outputs reliable after initial release.
- Hospitals might use the cost-tracking component to weigh quality gains against added compute expenses when choosing which AI agents to keep in production.
- Early heavy error feedback followed by later positive notes indicates the framework can build clinician trust over time rather than only at launch.
- Testing whether the rubric approach transfers to different medical specialties or note formats would reveal how broadly the governance method applies.
Load-bearing premise
Clinician-authored rubrics and live feedback entries give an unbiased and complete picture of clinical note quality that holds beyond the twenty participants and the cases they reviewed.
What would settle it
A replication with a larger and more diverse set of clinicians and patient cases in which quality scores fail to rise or live feedback stays dominated by error reports despite the same engineering interventions would show the governance approach does not produce reliable gains.
Figures





read the original abstract
Clinical AI systems require not just point-in-time evaluation but continuous governance: the ongoing practice of monitoring, evaluating, iterating, and re-evaluating performance throughout deployment. We present an end-to-end framework of governance that integrates rubric validation, live deployment feedback, technical performance monitoring, and cost tracking, with controlled experimentation gating system changes before deployment. Applied to Hyperscribe, an EHR-embedded agent that converts ambient audio into structured chart updates, twenty clinicians authored 1,646 validated rubrics across 823 cases. Seven Hyperscribe versions were evaluated through controlled experiments, with median scores improving from 84% to 95%. Analysis of 107 live feedback entries over three months showed feedback composition shifting from 79% error reports and 14% positive observations to 30% errors and 45% positive observations as engineering interventions resolved failures. Median processing time per audio segment was 8.1 seconds with a 99.6% effective completion rate after retry mechanisms absorbed transient model errors. These results demonstrate that continuous, multi-channel governance of deployed clinical AI is both achievable and effective.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper describes an end-to-end governance framework for Hyperscribe, an EHR-embedded AI agent that converts ambient audio into structured clinical notes. Twenty clinicians authored 1,646 validated rubrics across 823 cases to evaluate seven iterative versions of the system via controlled experiments, reporting median rubric scores rising from 84% to 95%. Analysis of 107 live feedback entries over three months showed a shift from 79% error reports to 45% positive observations. Technical metrics include 8.1-second median latency and 99.6% completion rate after retries. The authors conclude that continuous, multi-channel governance (rubric validation, live feedback, technical monitoring, cost tracking, and gated experimentation) is both achievable and effective for deployed clinical AI.
Significance. If the clinician rubrics and feedback reliably capture clinical note quality, the work offers a concrete, multi-channel example of post-deployment governance for AI in healthcare—an area where point-in-time evaluation is widely recognized as insufficient. The integration of rubric-based controlled experiments with live deployment logs and objective technical metrics provides a practical template that could inform regulatory and operational practices for clinical AI agents.
major comments (3)
- [Abstract and Results sections describing rubric and feedback analysis] The central claim that governance is 'effective' (Abstract and conclusion) rests on rubric-score improvements (84% to 95%) and feedback-composition shifts (79% errors to 45% positive). These metrics are generated entirely by the same 20 participating clinicians who authored the 1,646 rubrics and 107 feedback entries. No inter-rater reliability statistics, blinded independent review, or correlation with downstream clinical outcomes (e.g., note accuracy against gold-standard charts or patient outcomes) are reported, leaving open the possibility that observed gains reflect rater drift, selection effects, or expectation bias rather than genuine quality gains.
- [Results on rubric scores and live feedback] The manuscript reports directional improvements across seven versions but provides no statistical tests (e.g., Wilcoxon signed-rank or mixed-effects models accounting for clinician and case clustering) for the median score changes or feedback-composition shifts. Without these, it is unclear whether the reported gains exceed what would be expected from sampling variability or case-selection effects in the 823 cases.
- [Methods describing rubric creation and case selection] The 823 cases and 20 clinicians are described as the source of all rubrics and feedback, yet no details are given on case-selection criteria, potential selection bias, or how representative the sample is of broader clinical workflows. This directly affects the generalizability of the claim that the governance framework is effective beyond this specific deployment.
minor comments (2)
- [Abstract and Methods] The abstract and main text use 'median scores' and 'feedback composition' without specifying the exact rubric scale (e.g., binary pass/fail per item or continuous) or how positive/negative feedback was categorized, which would aid reproducibility.
- [Results on technical performance] Technical metrics (latency, completion rate) are presented as objective but the paper does not discuss how retry mechanisms or transient model errors were logged or whether they affected clinician-perceived quality.
Simulated Author's Rebuttal
We thank the referee for their constructive and detailed review of our manuscript on the end-to-end governance framework for Hyperscribe. The comments raise important points regarding the interpretation of our evaluation metrics, statistical rigor, and generalizability. We address each major comment below with clarifications drawn directly from the study design and indicate specific revisions to strengthen the manuscript.
read point-by-point responses
-
Referee: [Abstract and Results sections describing rubric and feedback analysis] The central claim that governance is 'effective' (Abstract and conclusion) rests on rubric-score improvements (84% to 95%) and feedback-composition shifts (79% errors to 45% positive). These metrics are generated entirely by the same 20 participating clinicians who authored the 1,646 rubrics and 107 feedback entries. No inter-rater reliability statistics, blinded independent review, or correlation with downstream clinical outcomes (e.g., note accuracy against gold-standard charts or patient outcomes) are reported, leaving open the possibility that observed gains reflect rater drift, selection effects, or expectation bias rather than genuine quality gains.
Authors: The evaluation design intentionally centers on structured, clinician-authored rubrics as the primary channel for assessing note quality in a real-world deployment, consistent with the multi-channel governance framework we describe. The 20 clinicians are practicing experts whose assessments directly inform system iterations. We agree, however, that the absence of inter-rater reliability statistics, blinded external review, and linkage to downstream clinical outcomes leaves room for alternative explanations such as rater drift or bias. We will add a dedicated Limitations section that explicitly discusses these issues, qualifies the scope of our effectiveness claims to the observed operational improvements within this framework, and notes the value of future studies incorporating such validations. revision: partial
-
Referee: [Results on rubric scores and live feedback] The manuscript reports directional improvements across seven versions but provides no statistical tests (e.g., Wilcoxon signed-rank or mixed-effects models accounting for clinician and case clustering) for the median score changes or feedback-composition shifts. Without these, it is unclear whether the reported gains exceed what would be expected from sampling variability or case-selection effects in the 823 cases.
Authors: We accept that formal statistical testing would improve the presentation of the iterative improvements. The medians were chosen to summarize the progression across controlled experiments with the same clinicians evaluating successive versions. In the revised manuscript we will add appropriate non-parametric tests (e.g., Wilcoxon signed-rank for paired version comparisons) and note any clustering considerations, thereby clarifying whether the observed shifts exceed sampling variability. revision: yes
-
Referee: [Methods describing rubric creation and case selection] The 823 cases and 20 clinicians are described as the source of all rubrics and feedback, yet no details are given on case-selection criteria, potential selection bias, or how representative the sample is of broader clinical workflows. This directly affects the generalizability of the claim that the governance framework is effective beyond this specific deployment.
Authors: We will expand the Methods section to detail the case-selection process, clinician recruitment criteria, inclusion/exclusion rules, and any steps taken to align the sample with typical clinical workflows. This addition will better support readers in assessing generalizability while acknowledging the single-site, real-world deployment context of the study. revision: yes
- The study did not collect inter-rater reliability statistics, blinded independent reviews, or correlations with downstream clinical outcomes; these cannot be supplied without additional data collection.
Circularity Check
No circularity: empirical results independent of internal definitions
full rationale
The paper reports measured improvements in rubric scores (84% to 95%) and feedback composition shifts from live deployment logs and clinician-authored rubrics across 1,646 entries. No equations, fitted parameters, derivations, or self-citations are present that reduce any claim to its own inputs by construction. The governance framework is evaluated through external controlled experiments and feedback analysis rather than self-referential definitions or renamed known results. This is a standard empirical evaluation with no load-bearing self-citation chains or ansatz smuggling.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Uptake of generative AI integrated with electronic health records in US hospitals.JAMA Netw Open
Everson J, Nong P, Richwine C. Uptake of generative AI integrated with electronic health records in US hospitals.JAMA Netw Open. 2025;8;(12):e2549463. doi:10.1001/jamanetworkopen.2025.49463
-
[2]
Physician survey on augmented intelligence
American Medical Association. Physician survey on augmented intelligence. Mar 2026. Available from www.ama-assn.org/system/files/physician-ai-sentiment-report.pdf
2026
-
[3]
Monitoring performance of clinical artificial intelligence in health care: a scoping review
Andersen ES, Hardt J, Nielsen C, et al. Monitoring performance of clinical artificial intelligence in health care: a scoping review.JBI Evidence Synthesis. 2024;22(12):2362–2419. doi:10.11124/JBIES-24-00042
-
[4]
HassanN,NayakA,GohE,etal.Addressingthechallengeofgovernance, risk, andcomplianceinrespon- sible AI.IEEE Engineering Management Review. 2024;52(3):90–100. doi:10.1109/EMR.2024.3407478
-
[5]
Evaluating clinical AI summaries with large language models as judges
Croxford E, Gao M, Pellegrini E, et al. Evaluating clinical AI summaries with large language models as judges.npj Digital Medicine. 2025;8:640. doi:10.1038/s41746-025-02005-2
-
[6]
Introducing HealthBench
Arora R, Chaurasia A, Pfeffer MA, et al. Introducing HealthBench. OpenAI; 2025. Available from: https://openai.com/index/healthbench/
2025
-
[7]
Tam TYC, Sivarajkumar S, Kapoor S, et al. A framework for human evaluation of large language models in healthcare derived from literature review.npj Digital Medicine. 2024;7:258. doi:10.1038/s41746-024- 01258-7
-
[8]
Wang W, et al. An evaluation framework for ambient digital scribing tools in clinical applications.npj Digital Medicine. 2025;8:358. doi:10.1038/s41746-025-01622-1
-
[9]
A general framework for governing marketed AI/ML medical devices.npj Digital Medicine
Babic B, et al. A general framework for governing marketed AI/ML medical devices.npj Digital Medicine. 2025;8:328. doi:10.1038/s41746-025-01717-9
-
[10]
Hyperscribe
Canvas Medical. Hyperscribe. 2025. Available from:https://canvasmedical.com/extensions/ hyperscribe
2025
-
[11]
canvas-hyperscribe
Canvas Medical. canvas-hyperscribe. GitHub; 2025. Available from:https://github.com/ canvas-medical/canvas-hyperscribe
2025
-
[12]
Canvas SDK Commands
Canvas Medical. Canvas SDK Commands. Available from:https://docs.canvasmedical.com/sdk/ commands/
-
[13]
Case-Specific Rubrics for Clinical AI Evaluation: Method- ology, Validation, and LLM-Clinician Agreement Across 823 Encounters
Shah A, Hines A, Downs A, Bajet D, et al. Case-Specific Rubrics for Clinical AI Evaluation: Method- ology, Validation, and LLM-Clinician Agreement Across 823 Encounters. [Companion paper–preprint pending] 17
-
[14]
Expert-Annotated Clinical Encounters: A Benchmark Dataset for Evaluating AI- Generated Medical Documentation
Shah A, et al. Expert-Annotated Clinical Encounters: A Benchmark Dataset for Evaluating AI- Generated Medical Documentation. PhysioNet. [To be added upon release]
-
[15]
Expert-Annotated Clinical Encounters: Dataset Usage
Shah A, et al. Expert-Annotated Clinical Encounters: Dataset Usage. GitHub; 2026. Available from: https://github.com/canvas-medical/dataset-usage
2026
-
[16]
Hussein R, Schein O, Bates DW, et al. Advancing healthcare AI governance through a comprehensive maturity model based on systematic review.npj Digital Medicine. 2026;9:236. doi:10.1038/s41746-026- 02418-7
-
[17]
Medical domain knowledge in domain-agnostic generative AI.npj Digital Medicine, 5(1):90, 2022
Wells BJ, Walji MF, Sittig DF, et al. A practical framework for appropriate implementation and review of artificial intelligence (FAIR-AI) in healthcare.npj Digital Medicine. 2025;8:514. doi:10.1038/s41746- 025-01900-y
-
[18]
Afshar M, Dligach D, Churpek MM, et al. A novel playbook for pragmatic trial operations to monitor and evaluate ambient artificial intelligence in clinical practice.NEJM AI. 2025;2(9). doi:10.1056/AIdbp2401267
-
[19]
Lukac, William Turner, Sitaram Vangala, Aaron T
Tierney AA, Sirek A, Ufere NN, et al. Randomized clinical trial of two ambient AI scribes for clinical documentation.NEJM AI. 2025. doi:10.1056/AIoa2501000
-
[20]
npj Digital Medicine 2025 8:1 8:274-
Asgari E, Fernandes M, Laranjo L, et al. A framework to assess clinical safety and hallucination rates of LLMs for medical text summarisation.npj Digital Medicine. 2025;8:274. doi:10.1038/s41746-025-01670-7 18
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.