Recognition: unknown
AG-TAL: Anatomically-Guided Topology-Aware Loss for Multiclass Segmentation of the Circle of Willis Using Large-Scale Multi-Center Datasets
Pith reviewed 2026-05-07 07:58 UTC · model grok-4.3
The pith
The AG-TAL loss improves multiclass segmentation of the Circle of Willis arteries by embedding anatomical priors for connectivity and boundary enforcement.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
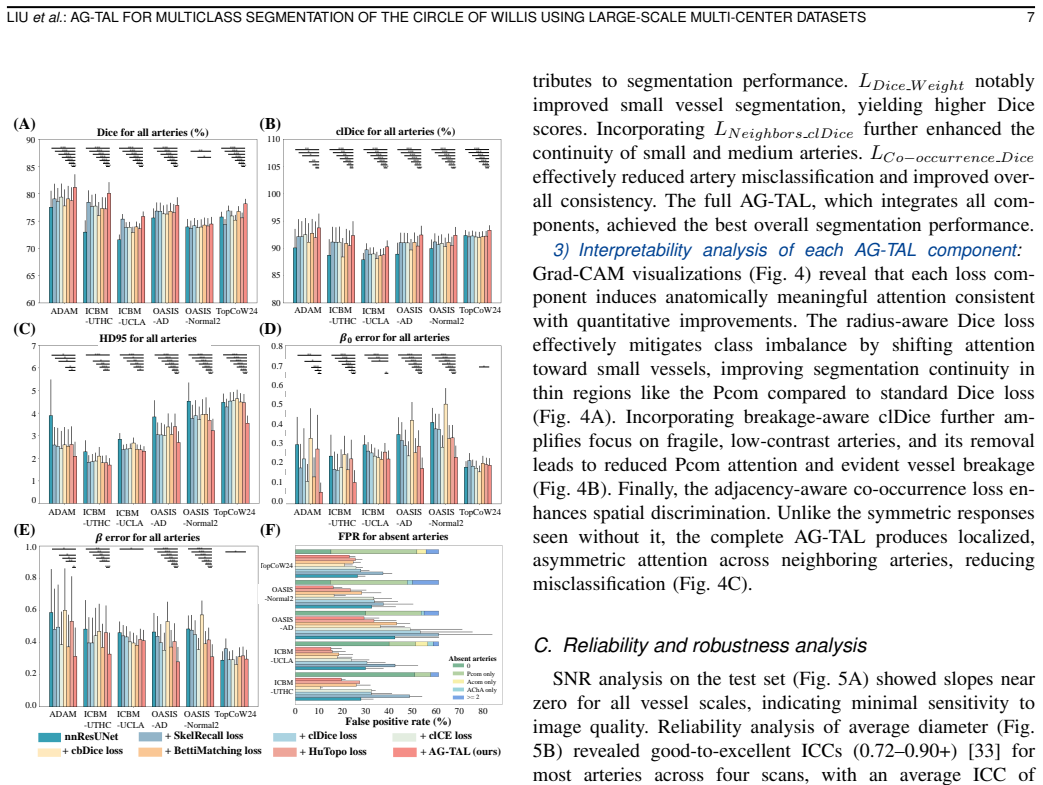
AG-TAL integrates a radius-aware Dice loss to counter class imbalance in small vessels, a breakage-aware clDice loss that uses group convolutions to preserve local connectivity efficiently, and an adjacency-aware co-occurrence loss that applies anatomical priors to enforce distinct boundaries between neighboring arteries. On 5-fold cross-validation it reaches an average Dice of 80.85 percent for all CoW arteries, with small-artery gains of 1.05 to 3.09 percent over prior methods. Across six independent datasets the scores range from 74.46 to 81.17 percent, showing 2.20 to 9.98 percent improvement on small arteries, and the same models support reliable biomarker extraction in an Alzheimer's-d
What carries the argument
Anatomically-Guided Topology-Aware Loss (AG-TAL) that combines radius-aware Dice, breakage-aware clDice via group convolutions, and adjacency-aware co-occurrence terms to enforce topology and anatomy.
If this is right
- Small arteries exhibit consistent accuracy gains, reducing misclassification of fine vascular branches.
- Performance remains stable across scanners and centers without additional fine-tuning.
- Vascular continuity is better preserved, lowering the rate of artificial breaks in the segmented network.
- The approach supports downstream clinical tasks such as morphological biomarker discovery in Alzheimer's cohorts.
- Unified multi-center annotations enable more robust training for future multiclass vascular models.
Where Pith is reading between the lines
- The same pattern of embedding anatomical priors into loss functions could be tested on other tubular structures such as coronary or pulmonary vessels.
- The released large-scale annotated CoW dataset may serve as a public benchmark for comparing topology-aware segmentation techniques.
- In clinical workflows the method could reduce manual correction time for pre-operative vascular maps.
- If the priors are made patient-specific or learned from data, the framework might handle congenital variants or severe pathology more gracefully.
Load-bearing premise
The anatomical adjacency priors and radius estimates used in the loss terms remain accurate and generalizable across patient populations and scanner variations.
What would settle it
Running the trained model on a new multi-center dataset whose vessel radii or adjacency statistics deviate markedly from the priors, and observing that small-artery Dice falls below baseline methods or that vessel discontinuities reappear.
Figures


read the original abstract
Accurate multiclass segmentation of the Circle of Willis (CoW) is essential for neurovascular disease management but remains challenging due to complex vascular topology and variable morphology. Existing deep learning methods often suffer from vascular discontinuities and inter-class misclassification, while current topological loss functions incur prohibitive computational costs in 3D multiclass settings. To address these limitations, we propose an Anatomically-Guided Topology-Aware Loss (AG-TAL) and introduce a large-scale, multi-center CoW dataset with unified annotations to facilitate robust model training. AG-TAL specifically integrates a radius-aware Dice loss to address class imbalance in small vessels, a breakage-aware clDice loss that utilizes group convolutions to efficiently preserve local connectivity, and an adjacency-aware co-occurrence loss that leverages anatomical priors to enforce distinct boundaries between neighboring arteries. Evaluated using 5-fold cross-validation, AG-TAL achieved an average Dice score of 80.85% for all CoW arteries, with small arteries notably higher by 1.05-3.09% compared to state-of-the-art methods. Across six independent datasets, the performance of AG-TAL achieved Dice scores ranging from 74.46% to 81.17% for all CoW arteries, with improvements of 2.20% to 9.98% for small arteries compared to other methods. This study demonstrates the superiority of AG-TAL in identifying multiclass CoW arteries and its ability to generalize well to multiple independent datasets. Furthermore, reliability analyses and clinical applications in an Alzheimer's disease cohort validate the AG-TAL's robustness and its potential for discovering imaging-based morphological biomarkers.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes AG-TAL, an anatomically-guided topology-aware loss for multiclass segmentation of Circle of Willis (CoW) arteries. AG-TAL combines a radius-aware Dice loss to handle small-vessel imbalance, a breakage-aware clDice loss using group convolutions for connectivity preservation, and an adjacency-aware co-occurrence loss that incorporates fixed anatomical priors to enforce distinct boundaries between neighboring arteries. The authors introduce a large-scale multi-center CoW dataset with unified annotations and report, via 5-fold cross-validation plus evaluation on six independent external datasets, an average Dice of 80.85% overall with 1.05-3.09% gains on small arteries versus state-of-the-art methods, plus Dice ranges of 74.46-81.17% on external data with 2.20-9.98% small-artery improvements. Additional reliability analyses and an Alzheimer's cohort application are mentioned to support robustness and biomarker potential.
Significance. If the central claims hold, the work offers a practical advance in topology-preserving segmentation for neurovascular imaging, where small arteries are particularly error-prone. The large multi-center training set and six-dataset external validation provide direct empirical support for generalization, which is a clear strength. The explicit construction of the loss from standard Dice/clDice terms plus anatomical weighting avoids circularity and supplies a reproducible baseline. These elements could influence loss design in other vascular or tubular-structure segmentation tasks if the anatomical priors prove robust across variants.
major comments (2)
- [Methods (AG-TAL formulation, adjacency-aware co-occurrence loss)] Methods (AG-TAL formulation, adjacency-aware co-occurrence loss): The loss employs fixed anatomical adjacency priors and radius estimates to penalize inter-class boundary violations. However, the Circle of Willis exhibits high topological variability (absent/hypoplastic segments in 40-50% of individuals). If the priors are derived from standard anatomy without adaptation or variant-specific handling, the term may systematically penalize valid configurations, especially for small arteries. This directly threatens the reported 1.05-3.09% gains and the 74.46-81.17% cross-dataset Dice range. The manuscript should either stratify results by variant status or demonstrate that the priors do not degrade performance on common variants.
- [Results and Experiments] Results and Experiments: The superiority claims rest on combined AG-TAL performance, yet the text does not isolate the contribution of each term via ablations (radius-aware Dice, breakage-aware clDice, adjacency-aware co-occurrence). Without these, it is impossible to determine whether the anatomical component drives the small-artery gains or whether simpler combinations suffice. In addition, no statistical significance tests (paired t-test, Wilcoxon, or similar with p-values and confidence intervals) are reported for the 1.05-3.09% and 2.20-9.98% improvements, leaving the magnitude of the effect uncertain.
minor comments (2)
- [Abstract] Abstract: The statement that AG-TAL 'generalize[s] well to multiple independent datasets' would be strengthened by briefly noting the total number of subjects or scans in the new multi-center dataset and the exact state-of-the-art baselines used for comparison.
- [Throughout] Throughout: Define 'small arteries' explicitly (e.g., list of vessel labels) on first use and maintain consistent terminology when reporting per-artery or per-group Dice scores.
Simulated Author's Rebuttal
We thank the referee for the constructive and insightful comments, which highlight important considerations for the robustness of AG-TAL. We address each major comment point by point below. We agree that the concerns are valid and will revise the manuscript to incorporate additional analyses, ablations, and statistical tests as detailed in our responses.
read point-by-point responses
-
Referee: Methods (AG-TAL formulation, adjacency-aware co-occurrence loss): The loss employs fixed anatomical adjacency priors and radius estimates to penalize inter-class boundary violations. However, the Circle of Willis exhibits high topological variability (absent/hypoplastic segments in 40-50% of individuals). If the priors are derived from standard anatomy without adaptation or variant-specific handling, the term may systematically penalize valid configurations, especially for small arteries. This directly threatens the reported 1.05-3.09% gains and the 74.46-81.17% cross-dataset Dice range. The manuscript should either stratify results by variant status or demonstrate that the priors do not degrade performance on common variants.
Authors: We acknowledge the well-known high topological variability of the Circle of Willis, including absent or hypoplastic segments in a substantial portion of the population. The adjacency-aware co-occurrence loss in AG-TAL incorporates fixed anatomical priors as soft, weighted penalties rather than rigid constraints, which in principle permits some deviation from standard configurations while still encouraging plausible boundaries. However, we agree that without explicit validation this leaves open the possibility of unintended penalization on variants, particularly affecting small arteries. In the revised manuscript we will add a stratification of results by variant status (inferable from the unified artery annotations, e.g., presence/absence of PComA or AComA segments) and include a dedicated supplementary analysis reporting Dice scores separately for variant versus non-variant cases across the internal and external datasets. This will directly demonstrate whether the reported small-artery gains are preserved under common anatomical variants. revision: yes
-
Referee: Results and Experiments: The superiority claims rest on combined AG-TAL performance, yet the text does not isolate the contribution of each term via ablations (radius-aware Dice, breakage-aware clDice, adjacency-aware co-occurrence). Without these, it is impossible to determine whether the anatomical component drives the small-artery gains or whether simpler combinations suffice. In addition, no statistical significance tests (paired t-test, Wilcoxon, or similar with p-values and confidence intervals) are reported for the 1.05-3.09% and 2.20-9.98% improvements, leaving the magnitude of the effect uncertain.
Authors: We agree that isolating the contribution of each loss term is necessary to substantiate the design choices and that statistical testing is required to assess the reliability of the observed improvements. In the revised manuscript we will add a full set of ablation experiments that disable each component in turn (radius-aware Dice, breakage-aware clDice, and adjacency-aware co-occurrence) while keeping the others fixed, reporting the resulting Dice scores with particular emphasis on small-artery performance. We will also perform and report paired statistical tests (e.g., paired t-tests or Wilcoxon signed-rank tests) with p-values and 95% confidence intervals on the per-fold and per-dataset improvements, using the 5-fold cross-validation results and the six external test sets. These additions will allow readers to evaluate the incremental value of the anatomical prior term. revision: yes
Circularity Check
AG-TAL constructed from standard losses plus external anatomical terms; no self-referential reduction
full rationale
The paper defines AG-TAL explicitly as the sum of three additive terms: a radius-aware Dice loss (to handle small-vessel imbalance), a breakage-aware clDice loss (using group convolutions for connectivity), and an adjacency-aware co-occurrence loss (using fixed anatomical priors for boundary enforcement). These are presented as direct extensions of the well-known Dice and clDice formulations, with the anatomical adjacency matrix and radius estimates supplied as external inputs rather than quantities fitted from the network outputs or derived from the loss itself. No equation in the provided text shows a central performance metric or loss component reducing by construction to a parameter estimated on the same data. Cross-dataset evaluation on six independent cohorts supplies external validation, confirming the derivation chain is self-contained against benchmarks.
Axiom & Free-Parameter Ledger
free parameters (1)
- loss-term weighting coefficients
axioms (2)
- domain assumption Anatomical adjacency relations among CoW arteries are stable and correctly annotated across the dataset
- domain assumption Group convolutions preserve local vessel connectivity without introducing topological artifacts
Reference graph
Works this paper leans on
-
[1]
Ischemic Strokes Due to Large-Vessel Occlusions Contribute Disproportionately to Stroke- Related Dependence and Death: A Review
K. Malhotra, J. Gornbein, and J. L. Saver, “Ischemic Strokes Due to Large-Vessel Occlusions Contribute Disproportionately to Stroke- Related Dependence and Death: A Review”,Front. Neurol., vol. 8, pp. 651, Nov. 2017
2017
-
[2]
The effect of intracranial stenosis on cognitive decline in a memory clinic cohort
M. J. R. Lim, C. S. Tan, B. Gyanwali, C. Chen, and S. Hilal, “The effect of intracranial stenosis on cognitive decline in a memory clinic cohort”, Eur . J. Neurol., vol. 28, no. 6, pp. 1829–1839, Jun. 2021
2021
-
[3]
Asymptomatic carotid stenosis is associated with mobility and cognitive dysfunction and heightens falls in older adults
V . L. Grayet al., “Asymptomatic carotid stenosis is associated with mobility and cognitive dysfunction and heightens falls in older adults”, J. V asc. Surg., vol. 71, no. 6, pp. 1930–1937, Jun. 2020
1930
-
[4]
eICAB: A novel deep learning pipeline for Circle of Willis multiclass segmentation and analysis
F. Dumaiset al., “eICAB: A novel deep learning pipeline for Circle of Willis multiclass segmentation and analysis”,NeuroImage, vol. 260, pp. 119425, Oct. 2022
2022
-
[5]
J. Houet al., “Relationship between Circle of Willis Variations and Cerebral or Cervical Arteries Stenosis Investigated by Computer To- mography Angiography and Multitask Convolutional Neural Network”, J. Healthc. Eng., vol. 2021, pp. 1–8, Oct. 2021
2021
-
[6]
nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation
F. Isensee, P. F. Jaeger, S. A. A. Kohl, J. Petersen, and K. H. Maier-Hein, “nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation”,Nat. methods, vol. 18, no. 2, pp. 203–211, Feb. 2021
2021
-
[7]
Topologically faithful multi-class segmentation in medical images,
A. H. Bergeret al., “Topologically faithful multi-class segmentation in medical images,” inProc. Int. Conf. Med. Image Comput. Comput.- Assist. Intervent. (MICCAI), Oct. 2024, pp. 721–731
2024
-
[8]
A Topological Loss Function for Deep-Learning Based Image Segmentation Using Persistent Homology
J. R. Clough, N. Byrne, I. Oksuz, V . A. Zimmer, J. A. Schnabel, and A. P. King, “A Topological Loss Function for Deep-Learning Based Image Segmentation Using Persistent Homology”,IEEE Trans. Pattern Anal. Mach. Intell., vol. 44, no. 12, pp. 8766–8778, Dec. 2022
2022
-
[9]
Topology-preserving deep image segmentation,
X. Hu, F. Li, D. Samaras, and C. Chen, “Topology-preserving deep image segmentation,” inAdvances in Neural Information Processing Systems (NeurIPS), Vancouver, BC, Canada, Dec. 2019
2019
-
[10]
Topologically faithful image segmentation via induced matching of persistence barcodes
N. Stucki, J. C. Paetzold, S. Shit, B. H. Menze, and U. Bauer, “Topologically faithful image segmentation via induced matching of persistence barcodes”, inProc. 40th Int. Conf. Mach. Learn. (ICML), LIUet al.: AG-TAL FOR MULTICLASS SEGMENTATION OF THE CIRCLE OF WILLIS USING LARGE-SCALE MULTI-CENTER DATASETS 11 Jul. 2023, pp. 32698–32727
2023
-
[11]
Efficient betti match- ing enables topology-aware 3D segmentation via persistent homology
N. Stucki, V . B¨urgin, J. C. Paetzold, and U. Bauer, “Efficient betti match- ing enables topology-aware 3D segmentation via persistent homology”, arXiv preprint arXiv:2407.04683, 2024
-
[12]
clDice - a Novel Topology-Preserving Loss Function for Tubular Structure Segmentation
S. Shitet al., “clDice - a Novel Topology-Preserving Loss Function for Tubular Structure Segmentation”, inProc. IEEE/CVF Conf. Comput. Vis. Pattern Recognit. (CVPR), Nashville, TN, USA, Jun. 2021, pp. 16555–16564
2021
-
[13]
A skeletonization algorithm for gradient-based optimization,
M. J. Mentenet al., “A skeletonization algorithm for gradient-based optimization,” inProc. IEEE/CVF Int. Conf. Comput. Vis. (ICCV), 2023, pp. 21394–21403
2023
-
[14]
Centerline boundary dice loss for vascular segmentation,
P. Shiet al., “Centerline boundary dice loss for vascular segmentation,” inInt. Conf. Med. Image Comput. Comput.-Assist. Intervent. (MICCAI), Cham, Switzerland: Springer Nature Switzerland, 2024, pp. 46–56
2024
-
[15]
The centerline- cross entropy loss for vessel-like structure segmentation: Better topology consistency without sacrificing accuracy,
C. Acebes, A. H. Moustafa, O. Camara, and A. Galdran, “The centerline- cross entropy loss for vessel-like structure segmentation: Better topology consistency without sacrificing accuracy,” inInt. Conf. Med. Image Com- put. Comput.-Assist. Intervent. (MICCAI), Cham, Switzerland: Springer Nature Switzerland, 2024, pp. 710–720
2024
-
[16]
Skeleton recall loss for connectivity conserving and resource efficient segmentation of thin tubular structures,
Y . Kirchhoffet al., “Skeleton recall loss for connectivity conserving and resource efficient segmentation of thin tubular structures,” inProc. Eur . Conf. Comput. Vis. (ECCV), Cham, Switzerland: Springer Nature Switzerland, 2024, pp. 218–234
2024
-
[17]
Edelsbrunner,Computational topology: an introduction
H. Edelsbrunner,Computational topology: an introduction. in Miscella- neous Books, vol. 69. Providence, R.I: American Mathematical Society, 2010
2010
-
[18]
Available: https://adam.isi.uu.nl/
UMC Utrecht,Aneurysm Detection And segMentation Challenge (ADAM) 2020, [Online]. Available: https://adam.isi.uu.nl/. Accessed: Oct. 16, 2025
2020
-
[19]
Digital reconstruction and morphometric analysis of human brain arterial vasculature from magnetic resonance angiography
S. N. Wrightet al., “Digital reconstruction and morphometric analysis of human brain arterial vasculature from magnetic resonance angiography”, NeuroImage, vol. 82, pp. 170–181, Nov. 2013
2013
-
[20]
Towards Automated Brain Aneurysm Detection in TOF-MRA: Open Data, Weak Labels, and Anatomical Knowledge
T. Di Notoet al., “Towards Automated Brain Aneurysm Detection in TOF-MRA: Open Data, Weak Labels, and Anatomical Knowledge”, Neuroinformatics, vol. 21, no. 1, pp. 21–34, Jan. 2023
2023
-
[21]
A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM),
Mazziottaet al., “A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM),” Philos. Trans. R. Soc. Lond. B, Biol. Sci., vol. 356, pp. 1293–1322, 2001
2001
-
[22]
Available: https://brain-development.org/ixi-dataset/
Imperial College London,IXI Dataset – Brain Development, [Online]. Available: https://brain-development.org/ixi-dataset/. Accessed: Oct. 16, 2025
2025
-
[23]
The effects of healthy aging on intracerebral blood ves- sels visualized by magnetic resonance angiography,
E. Bullittet al., “The effects of healthy aging on intracerebral blood ves- sels visualized by magnetic resonance angiography,”Neurobiol. Aging, vol. 31, no. 2, pp. 290–300, Feb. 2010
2010
-
[24]
OASIS-3: Longitudinal neuroimaging, clin- ical, and cognitive dataset for normal aging and Alzheimer disease,
P. J. LaMontagneet al., “OASIS-3: Longitudinal neuroimaging, clin- ical, and cognitive dataset for normal aging and Alzheimer disease,” Radiology and Imaging, Dec. 15, 2019
2019
-
[25]
K. Yanget al., “Benchmarking the CoW with the TopCoW Challenge: Topology-aware anatomical segmentation of the Circle of Willis for CTA and MRA,”arXiv preprint arXiv:2312.17670, 2023
-
[26]
Precision functional mapping of individual human brains,
E. M. Gordonet al., “Precision functional mapping of individual human brains,”Neuron, vol. 95, no. 4, pp. 791–807, 2017
2017
-
[27]
B. B. Avants,ANTs Wiki, GitHub repository. [Online]. Available: https://github.com/ANTsX/ANTs/wiki. Accessed: Oct. 16, 2025
2025
-
[28]
Highly accurate, automated quantification of 2D/3D orientation for cerebrovasculature using window optimizing method,
J. Menget al., “Highly accurate, automated quantification of 2D/3D orientation for cerebrovasculature using window optimizing method,”J. Biomed. Opt., vol. 27, 2022
2022
-
[29]
Co-occurrent features in semantic segmentation,
H. Zhang, H. Zhang, C. Wang, and J. Xie, “Co-occurrent features in semantic segmentation,” inProc. IEEE/CVF Conf. Comput. Vis. Pattern Recognit. (CVPR), 2019, pp. 548–557
2019
-
[30]
Swin UNETR: Swin transformers for semantic segmentation of brain tumors in MRI images,
A. Hatamizadehet al., “Swin UNETR: Swin transformers for semantic segmentation of brain tumors in MRI images,” inInt. MICCAI Brain- lesion Workshop, Cham, Switzerland: Springer International Publishing, 2021, pp. 272–284
2021
-
[31]
U-mamba: Enhancing long-range dependency for biomedical image segmentation
J. Ma, F. Li, and B. Wang, “U-Mamba: Enhancing long-range dependency for biomedical image segmentation,”arXiv preprint arXiv:2401.04722, 2024
-
[32]
Grad-CAM: Visual explanations from deep networks via gradient-based localization,
R. R. Selvarajuet al., “Grad-CAM: Visual explanations from deep networks via gradient-based localization,” inProc. IEEE Int. Conf. Comput. Vis. (ICCV), 2017, pp. 618–626
2017
-
[33]
A guideline of selecting and reporting intraclass correlation coefficients for reliability research,
T. K. Koo and M. Y . Li, “A guideline of selecting and reporting intraclass correlation coefficients for reliability research,”J. Chiropr . Med., vol. 15, no. 2, pp. 155–163, Jun. 2016
2016
-
[34]
FFCM-MRF: An accurate and generalizable cerebrovas- cular segmentation pipeline for humans and rhesus monkeys based on TOF-MRA,
Y . Cuiet al., “FFCM-MRF: An accurate and generalizable cerebrovas- cular segmentation pipeline for humans and rhesus monkeys based on TOF-MRA,”Comput. Biol. Med., vol. 170, p. 107996, 2024
2024
-
[35]
Loss odyssey in medical image segmentation,
J. Maet al., “Loss odyssey in medical image segmentation,”Med. Image Anal., vol. 71, p. 102035, Jul. 2021
2021
-
[36]
Loss functions in the era of semantic segmentation: A survey and outlook,
R. Azadet al., “Loss functions in the era of semantic segmentation: A survey and outlook,”arXiv preprint arXiv:2312.05391, 2023
-
[37]
Medical image segmentation review: The success of U-Net,
R. Azadet al., “Medical image segmentation review: The success of U-Net,”IEEE Trans. Pattern Anal. Mach. Intell., 2024
2024
-
[38]
Reducing the Hausdorff distance in medical image segmentation with convolutional neural networks,
D. Karimi and S. E. Salcudean, “Reducing the Hausdorff distance in medical image segmentation with convolutional neural networks,”IEEE Trans. Med. Imaging, vol. 39, no. 2, pp. 499–513, Feb. 2020
2020
-
[39]
Boundary loss for highly unbalanced segmentation,
H. Kervadecet al., “Boundary loss for highly unbalanced segmentation,” Med. Image Anal., vol. 67, p. 101851, Jan. 2021
2021
-
[40]
Segmentation of mediastinal lymph nodes in CT with anatomical priors,
T. S. Mathai, B. Liu, and R. M. Summers, “Segmentation of mediastinal lymph nodes in CT with anatomical priors,”Int. J. Comput. Assist. Radiol. Surg., vol. 19, no. 8, pp. 1537–1544, May 2024
2024
-
[41]
Removing segmentation inconsistencies with semi-supervised non-adjacency con- straint,
P.-A. Ganaye, M. Sdika, B. Triggs, and H. Benoit-Cattin, “Removing segmentation inconsistencies with semi-supervised non-adjacency con- straint,” Med. Image Anal., vol. 58, Art. no. 101551, 2019
2019
-
[42]
Research on melanoma image segmentation by incorporating medical prior knowledge,
H. Zhao, A. Wang, and C. Zhang, “Research on melanoma image segmentation by incorporating medical prior knowledge,”PeerJ Comput. Sci., vol. 8, p. e1122, Oct. 2022
2022
-
[43]
Novel imaging markers for altered cerebrovascular morphology in aging, stroke, and Alzheimer’s disease,
A. Deshpandeet al., “Novel imaging markers for altered cerebrovascular morphology in aging, stroke, and Alzheimer’s disease,”J. Neuroimaging, vol. 32, no. 5, pp. 956–967, Sep. 2022
2022
-
[44]
CF-loss: Clinically-relevant feature optimised loss function for retinal multi-class vessel segmentation and vascular feature measurement,
Y . Zhouet al., “CF-loss: Clinically-relevant feature optimised loss function for retinal multi-class vessel segmentation and vascular feature measurement,”Med. Image Anal., vol. 93, p. 103098, Apr. 2024
2024
-
[45]
Quantitative analysis of cerebral vasculature and its clinical effect on cognitive change in Alzheimer’s dementia and mild cognitive impairment,
T. Kimet al., “Quantitative analysis of cerebral vasculature and its clinical effect on cognitive change in Alzheimer’s dementia and mild cognitive impairment,”J. Neurol. Sci., vol. 476, p. 123598, Sep. 2025
2025
-
[46]
Intracranial stenosis and longitudinal progression of Alzheimer’s disease pathologies,
K. M. Kanget al., “Intracranial stenosis and longitudinal progression of Alzheimer’s disease pathologies,”Alzheimers Dement., vol. 21, no. 12, p. e71010, Dec. 2025
2025
-
[47]
Arterial spin labeling blood flow MRI: Its role in the early characterization of Alzheimer’s disease,
D. C. Alsop, W. Dai, M. Grossman, and J. A. Detre, “Arterial spin labeling blood flow MRI: Its role in the early characterization of Alzheimer’s disease,”J. Alzheimers Dis., vol. 20, no. 3, pp. 871–880, May 2010
2010
-
[48]
Assessment of cerebral blood flow in Alzheimer’s disease by spin-labeled magnetic resonance imaging,
D. C. Alsop, J. A. Detre, and M. Grossman, “Assessment of cerebral blood flow in Alzheimer’s disease by spin-labeled magnetic resonance imaging,”Ann. Neurol., vol. 47, no. 1, pp. 93–100, Jan. 2000
2000
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.