Recognition: no theorem link
VISTA: A Benchmark for Real-Time Video Streaming under Network Impairments in Surgical Teleoperation
Pith reviewed 2026-05-12 01:37 UTC · model grok-4.3
The pith
Network impairments reduce surgical teleoperation success from 97% in hospital LAN to 12% in GEO satellite conditions.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
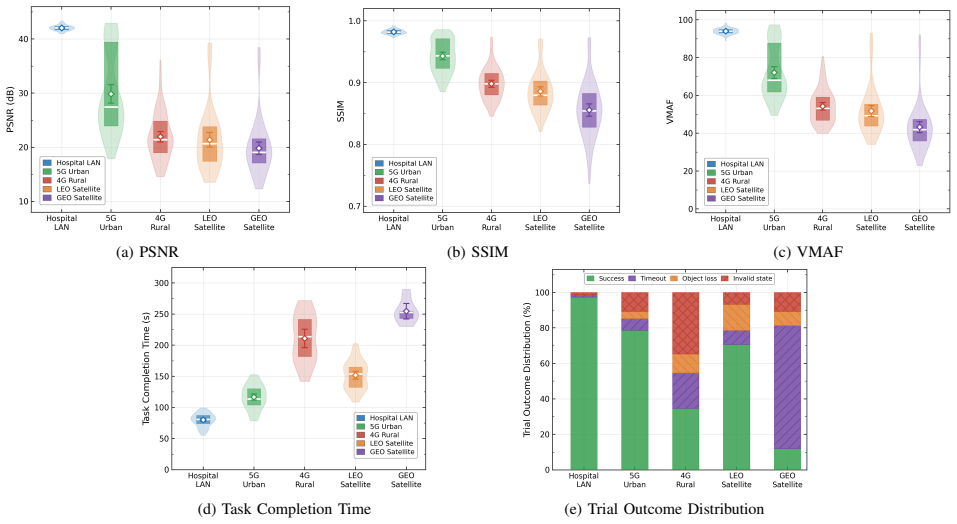
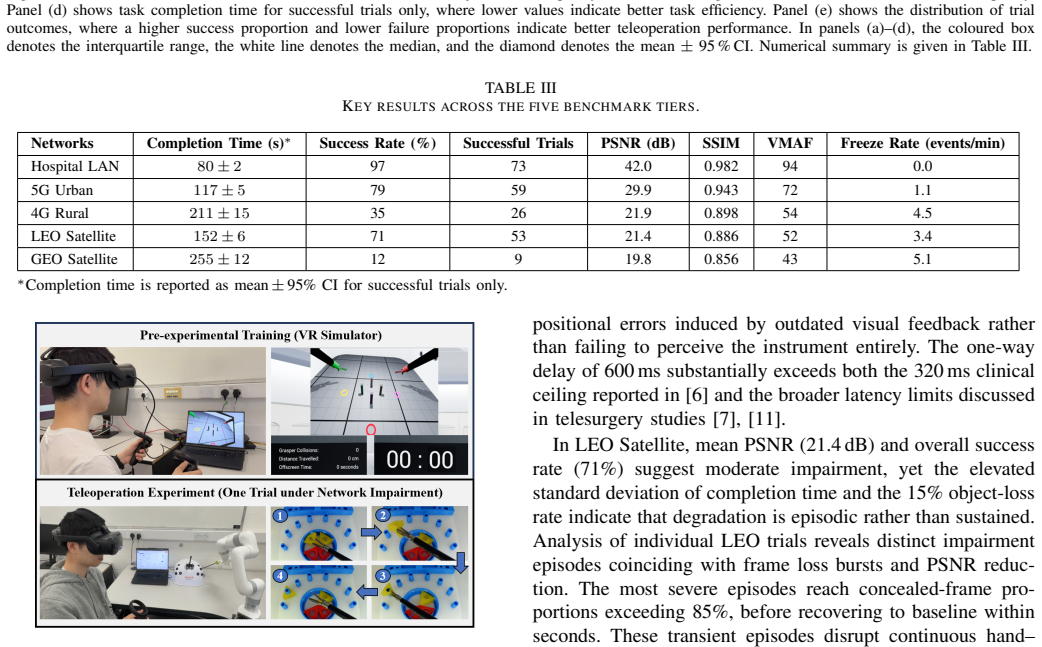
VISTA integrates a standardized peg transfer task with synchronized measurements of network quality of service, objective video quality through PSNR, SSIM and VMAF, and temporal continuity through freeze rate, while keeping a stable reverse control channel. Under emulated Hospital LAN, 5G Urban, 4G Rural, LEO Satellite and GEO Satellite profiles the benchmark records success rates falling from 97% to 79%, 35%, 71% and 12% respectively, with mean completion times for successful trials rising from 80 s to 117 s, 211 s, 152 s and 255 s.
What carries the argument
The VISTA benchmark, which uses Linux Traffic Control together with NetEm and the Gilbert-Elliott loss model to generate repeatable forward-path impairments while collecting multi-modal data on QoS, video quality and operator task performance.
If this is right
- Video streaming pipelines for teleoperation must maintain low freeze rates even under high-loss satellite profiles to preserve task success.
- Minimum network specifications for remote surgery can be derived by comparing the measured performance across the five emulated profiles.
- Objective video quality scores such as VMAF show correlation with human task completion under these impairments.
- Reproducible emulation enables direct comparison of alternative codecs or transport protocols without requiring physical network access.
- LEO satellite links support substantially higher success rates than GEO links for the same task.
Where Pith is reading between the lines
- Adaptive streaming techniques could be tested inside the same benchmark to quantify how much they offset the observed drops in success rate.
- Extending the task set beyond peg transfer would show whether more complex or time-critical procedures suffer even larger performance losses.
- The benchmark data could guide prioritization of low-latency links over raw bandwidth in the design of future medical networks.
- Real packet traces captured at actual surgical sites could later replace the synthetic loss model to increase ecological validity.
Load-bearing premise
The five emulated network conditions created with NetEm and the Gilbert-Elliott loss model accurately represent the impairments that occur in real surgical teleoperation deployments.
What would settle it
Repeating the peg transfer trials over live rather than emulated 4G rural or GEO satellite links and checking whether the observed success rates and completion times match the reported 35% and 12% figures.
Figures


read the original abstract
Real-time video streaming is crucial in surgical teleoperation, yet reproducible evaluation under realistic network impairments remains limited. This paper presents VISTA, a benchmark designed to study how impairments along the forward video path affect received video quality, temporal continuity, and human task performance. VISTA employs Linux Traffic Control with NetEm and a Gilbert-Elliott loss model to emulate five network conditions: Hospital LAN, 5G Urban, 4G Rural, LEO Satellite, and GEO Satellite. The benchmark integrates a standardised peg transfer task with synchronized measurements of network quality of service (QoS), objective video quality (PSNR, SSIM, and VMAF), and temporal continuity through freeze rate, while maintaining a stable reverse control channel. Across 375 experimental trials, network degradation substantially reduced teleoperation performance: success rate decreased from 97% in Hospital LAN to 79% in 5G Urban, 35% in 4G Rural, 71% in LEO Satellite, and 12% in GEO Satellite, while mean task completion time for successful trials increased from 80 s in Hospital LAN to 117 s in 5G Urban, 211 s in 4G Rural, 152 s in LEO Satellite, and 255 s in GEO Satellite. These findings show that network impairments have a direct impact on task completion and success in surgical teleoperation, and provide a reproducible basis for evaluating teleoperation video under realistic network constraints. Source code available at https://github.com/Dzxx623/VISTA.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces VISTA, a benchmark for real-time video streaming in surgical teleoperation. It emulates five network conditions (Hospital LAN, 5G Urban, 4G Rural, LEO Satellite, GEO Satellite) via NetEm and the Gilbert-Elliott loss model, integrates a standardized peg-transfer task, and reports synchronized QoS, objective video quality (PSNR, SSIM, VMAF), freeze rate, and human performance metrics across 375 trials. Key findings include success-rate drops from 97% (Hospital LAN) to 12% (GEO Satellite) and corresponding increases in mean completion time for successful trials.
Significance. If the results hold, VISTA supplies a reproducible, publicly coded empirical benchmark that quantifies the sensitivity of surgical teleoperation to forward-path network impairments. The use of standard tools, a fixed task, and direct measurement of both objective video metrics and task outcomes strengthens its utility for the community and supports the central claim of direct performance impact.
major comments (1)
- Network Emulation section: the claim that the five NetEm/Gilbert-Elliott profiles represent realistic surgical teleoperation impairments rests on parameter selection without reported validation against field traces from actual operating-room or remote-surgery deployments; this assumption is load-bearing for the benchmark's claimed applicability.
minor comments (2)
- Abstract: the summary omits the number of participants/operators, whether trial order was randomized, and any statistical tests or confidence intervals supporting the reported success-rate and time differences.
- Results presentation: tables or figures reporting per-condition success rates and completion times should include standard deviations or inter-quartile ranges to convey variability across the 375 trials.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and the recommendation for minor revision. We address the major comment point by point below.
read point-by-point responses
-
Referee: Network Emulation section: the claim that the five NetEm/Gilbert-Elliott profiles represent realistic surgical teleoperation impairments rests on parameter selection without reported validation against field traces from actual operating-room or remote-surgery deployments; this assumption is load-bearing for the benchmark's claimed applicability.
Authors: We agree that the original manuscript does not report direct validation of the chosen parameters against field traces collected from actual surgical teleoperation deployments. Such traces are not publicly available, and collecting them would require access to operational remote-surgery systems that was outside the scope of this work. The five profiles were instead constructed from standard latency, jitter, bandwidth, and loss values drawn from the networking literature for the respective environments (Hospital LAN, 5G urban, 4G rural, LEO, and GEO satellite). In the revised manuscript we will (i) explicitly cite the literature sources used for each parameter set, (ii) describe the Gilbert-Elliott model configuration in greater detail, and (iii) add a limitations paragraph that qualifies the applicability claim and notes the absence of surgical-specific field validation. These changes make the parameter-selection process transparent and address the load-bearing assumption without overstating the realism of the emulation. revision: partial
Circularity Check
No significant circularity; purely empirical benchmark
full rationale
The paper reports direct experimental measurements from 375 controlled trials using NetEm/Gilbert-Elliott emulations on a peg-transfer task. Success rates, completion times, PSNR/SSIM/VMAF, and freeze rates are measured outcomes, not derived via equations, fitted parameters, or predictions that reduce to prior definitions. No load-bearing self-citations, ansatzes, or uniqueness theorems appear in the central claims. The study is self-contained against its stated experimental conditions and external benchmarks.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
J. G. Meara, A. J. M. Leather, L. Hagander, B. C. Alkire, N. Alonso, E. A. Ameh, S. W. Bickler, L. Conteh, A. J. Dare, J. Davies,et al., “Global Surgery 2030: evidence and solutions for achieving health, wel- fare, and economic development,”Lancet, vol. 386, no. 9993, pp. 569– 624, 2015
work page 2030
-
[2]
Transatlantic robot-assisted telesurgery,
J. Marescaux, J. Leroy, M. Gagner, F. Rubino, D. Mutter, M. Vix, S. E. Butner, and M. K. Smith, “Transatlantic robot-assisted telesurgery,” Nature, vol. 413, no. 6854, pp. 379–380, 2001
work page 2001
-
[3]
B. Rocco, M. C. Moschovas, S. Saikali, G. Gaia, V . Patel, and M. C. Sighinolfi, “Insights from telesurgery expert conference on recent clinical experience and current status of remote surgery,”Journal of Robotic Surgery, vol. 18, no. 1, p. 240, 2024
work page 2024
-
[4]
H. Akasaka, K. Hakamada, H. Morohashi, T. Kanno, K. Kawashima, Y . Ebihara, E. Oki, S. Hirano, and M. Mori, “Impact of the suboptimal communication network environment on telerobotic surgery performance and surgeon fatigue,”PLoS One, vol. 17, no. 6, p. e0270039, 2022
work page 2022
-
[5]
Service requirements for Video, Imaging and Audio for Profes- sional Applications (VIAPA),
3GPP, “Service requirements for Video, Imaging and Audio for Profes- sional Applications (VIAPA),”3GPP TS 22.263, Release 19, 2025
work page 2025
-
[6]
Y . Wang, Q. Ai, T. Shi, B. Gao, W. Zhao, C. Jiang, G. Liu, L. Zhang, H. Li, et al., “Influence of network latency and bandwidth on robot- assisted laparoscopic telesurgery: A pre-clinical experiment,”Chinese Medical Journal, vol. 138, no. 3, pp. 325–331, 2025
work page 2025
-
[7]
Telesurgery: current status and strategies for latency reduction,
Z. Y . Motiwala, A. Desai, R. Bisht, S. Lathkar, S. Misra, and D. D. Carbin, “Telesurgery: current status and strategies for latency reduction,” J. Robot. Surg., vol. 19, no. 1, p. 153, 2025
work page 2025
-
[8]
Analyzing Real-time Video Delivery over Cellular Networks for Remote Piloting Aerial Vehicles,
A. Baltaci, H. Cech, N. Mohan, F. Geyer, V . Bajpai, J. Ott, and D. Schupke, “Analyzing Real-time Video Delivery over Cellular Networks for Remote Piloting Aerial Vehicles,” inProc. ACM Internet Measure- ment Conference (IMC), 2022, pp. 98–112
work page 2022
-
[9]
TeleSim: A Network-Aware Testbed and Benchmark Dataset for Telerobotic Applications
Z. Deng, Z. Yuan, and L. Zou, “TeleSim: A Network-Aware Testbed and Benchmark Dataset for Telerobotic Applications,”arXiv preprint arXiv:2507.04425, 2025
work page internal anchor Pith review arXiv 2025
-
[10]
J. M. Thompson, M. P. Ottensmeyer, and T. B. Sheridan, “Human factors in telesurgery: Effects of time delay and asynchrony in video and control feedback with local manipulative assistance,”Telemedicine Journal, vol. 5, no. 2, pp. 129–137, 1999
work page 1999
-
[11]
S. Xu, M. Perez, K. Yang, C. Perrenot, J. Felblinger, and J. Hubert, “Determination of the latency effects on surgical performance and the acceptable latency levels in telesurgery using the dV-Trainer® simulator,”Surg. Endosc., vol. 28, no. 9, pp. 2569–2576, Sep. 2014, doi: 10.1007/s00464-014-3504-z
-
[12]
A. Kumcu, L. Vermeulen, S. A. Elprama, P. Duysburgh, L. Plati ˇsa, Y . Van Nieuwenhove, N. Van De Winkel, A. Jacobs, J. Van Looy, and W. Philips, “Effect of video lag on laparoscopic surgery: correlation between performance and usability at low latencies,”Int. J. Med. Robot. Comput. Assist. Surg., vol. 13, no. 2, Art. no. e1758, 2017, doi: 10.1002/rcs.1758
-
[13]
tc-netem(8) — Linux manual page,
F. Ludovici and H. P. Pfeifer, “tc-netem(8) — Linux manual page,” man7.org. [Online]. Available: https://www.man7.org/linux/man-pages/ man8/tc-netem.8.html. Accessed: Mar. 14, 2026
work page 2026
-
[14]
Capacity of a burst-noise channel,
E. N. Gilbert, “Capacity of a burst-noise channel,”Bell Syst. Tech. J., vol. 39, no. 5, pp. 1253–1265, 1960
work page 1960
-
[15]
The Gilbert–Elliott model for packet loss in real-time services on the Internet,
G. Haßlinger and O. Hohlfeld, “The Gilbert–Elliott model for packet loss in real-time services on the Internet,” inProc. 14th GI/ITG Conf. Meas., Model. Eval. Comput. Commun. Syst. (MMB), Dortmund, Germany, 2008, pp. 1–15
work page 2008
-
[16]
Network performance objectives for IP-based services,
ITU-T, “Network performance objectives for IP-based services,”ITU-T Rec. Y.1541, 2011
work page 2011
-
[17]
Service requirements for the 5G system,
3GPP, “Service requirements for the 5G system,”3GPP TS 22.261, Release 17
-
[18]
Breaking Through the Clouds: Performance Insights into Starlink’s Latency and Packet Loss,
R. Richter, V . Ververis, and V . Bajpai, “Breaking Through the Clouds: Performance Insights into Starlink’s Latency and Packet Loss,” inIFIP Networking Conference (Networking), 2025
work page 2025
- [19]
-
[20]
A systematic review of virtual reality simulators for robot-assisted surgery,
A. Moglia, V . Ferrari, L. Morelli, M. Ferrari, F. Mosca, and A. Cuschieri, “A systematic review of virtual reality simulators for robot-assisted surgery,”Eur. Urol., vol. 69, no. 6, pp. 1065–1080, 2016
work page 2016
-
[21]
N. J. Hogle, W. D. Widmann, A. O. Ude, M. A. Hardy, and D. L. Fowler, “Does training novices to criteria and does rapid acquisition of skills on laparoscopic simulators have predictive validity or are we just playing video games?,”J. Surg. Educ., vol. 65, no. 6, pp. 431–435, 2008
work page 2008
-
[22]
x264 — a free H.264/A VC encoder,
VideoLAN Organization, “x264 — a free H.264/A VC encoder,” [On- line]. Available: https://www.videolan.org/developers/x264.html. Ac- cessed: Mar. 14, 2026
work page 2026
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.