Recognition: no theorem link
Annotation-free deep learning for detection and segmentation of fetal germinal matrix-intraventricular hemorrhage in brain MRI
Pith reviewed 2026-05-12 04:46 UTC · model grok-4.3
The pith
An annotation-free deep learning model detects and segments fetal brain hemorrhages on MRI by training only on synthesized pseudo-images.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
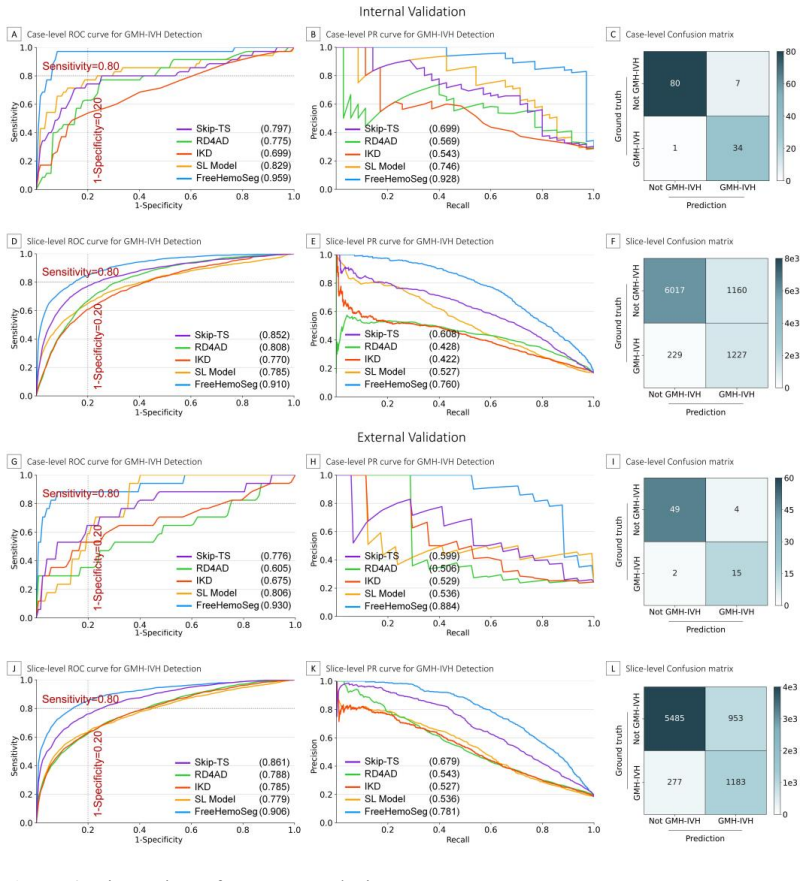
FreeHemoSeg is an annotation-free deep learning framework trained solely on pseudo GMH-IVH images synthesized from normal fetal T2-weighted MRI data according to medical priors; on held-out real cases it reaches internal sensitivity 0.914 and specificity 0.966 with DSC 0.559, external sensitivity 0.824 and specificity 0.943 with DSC 0.512, outperforming both supervised and unsupervised baselines and improving radiologist performance when used as assistance.
What carries the argument
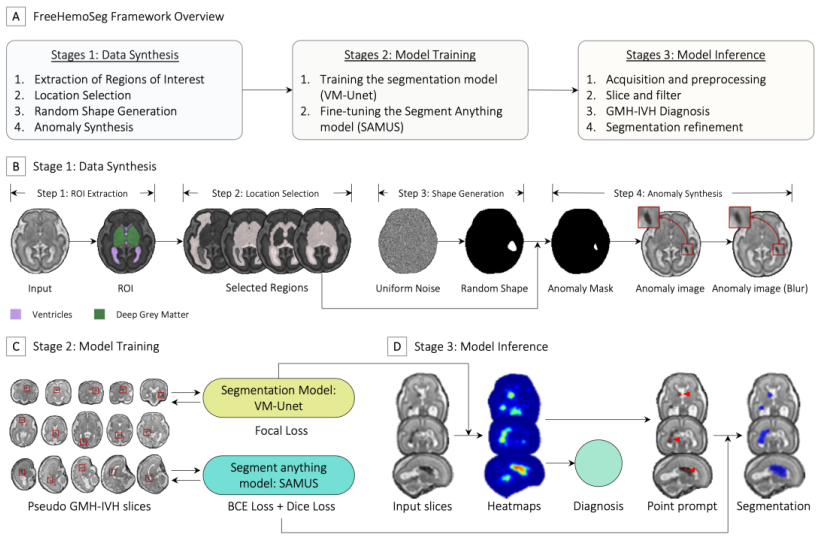
Synthesis of pseudo GMH-IVH images from normal fetal MRI scans guided by medical priors on hemorrhage site and signal characteristics, which then serve as the sole training data for the FreeHemoSeg detection and segmentation network.
If this is right
- Automated detection and segmentation of fetal brain hemorrhages becomes feasible without any manual annotations.
- Radiologists achieve higher sensitivity and greater diagnostic confidence while spending less time per case.
- Performance remains strong across data collected at multiple hospitals.
- Earlier and more consistent identification of GMH-IVH can support timely clinical decisions.
Where Pith is reading between the lines
- Medical priors can substitute for scarce annotations when building AI systems for rare fetal imaging findings.
- The synthesis strategy may extend to other low-prevalence prenatal or pediatric brain conditions.
- Lowering the annotation barrier could speed development of diagnostic tools for uncommon medical events.
Load-bearing premise
Pseudo hemorrhage images created from normal scans using medical priors resemble real GMH-IVH closely enough that a model trained on them will generalize to actual clinical cases.
What would settle it
FreeHemoSeg is evaluated on a large independently annotated collection of real GMH-IVH cases and shows substantially lower sensitivity or specificity than the reported validation numbers.
Figures




read the original abstract
Background: Prenatal germinal matrix-intraventricular hemorrhage (GMH-IVH) is a leading cause of infant mortality and neurodevelopmental impairment. Manual diagnosis and lesion segmentation are labor-intensive and error-prone. Deep learning models offer potential for automation but typically require large annotated datasets, which are challenging to obtain. Purpose: To develop and validate an annotation-free deep learning framework for automated detection and segmentation of GMH-IVH on brain MRI. Materials and Methods: This retrospective study analyzed 2D T2-weighted MRI data from pregnant women collected from October 2015 to October 2023 at one hospital (internal validation) and two hospitals (external validation). Eligible participants included healthy fetuses and those with GMH-IVH. FreeHemoSeg was developed and trained using pseudo GMH-IVH images synthesized from normal fetal data guided by medical priors. Primary outcomes included diagnostic accuracy (area under the ROC curve [AUROC], sensitivity, specificity) and segmentation accuracy (Dice similarity coefficient [DSC]). A reader study evaluated clinical utility. Results: A total of 1674 stacks from 558 pregnant women were analyzed. FreeHemoSeg achieved the highest performance in both internal (sensitivity: 0.914, 95% CI 0.869-0.945; specificity: 0.966, 95% CI 0.946-0.978; DSC: 0.559, 95% CI 0.546-0.571) and external validation (sensitivity: 0.824, 95% CI 0.739-0.885; specificity: 0.943, 95% CI 0.913-0.964; DSC: 0.512, 95% CI 0.497-0.526), outperforming supervised and unsupervised methods. FreeHemoSeg assistance improved radiologists' sensitivity (from 0.882 to 0.941-1.000) and diagnostic confidence while reducing interpretation time by 16.0-52.7%. Conclusion: FreeHemoSeg accurately detects and localizes fetal brain hemorrhages without annotated training data, enabling earlier diagnosis and supporting timely clinical management.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents FreeHemoSeg, an annotation-free deep learning framework for automated detection and segmentation of fetal GMH-IVH on T2-weighted brain MRI. The model is trained exclusively on pseudo-GMH-IVH images synthesized from normal fetal scans using medical priors, then evaluated on internal (one hospital) and external (two hospitals) retrospective datasets of 1674 stacks from 558 pregnant women. It reports strong diagnostic performance (internal sensitivity 0.914/specificity 0.966; external 0.824/0.943) with moderate segmentation (DSC 0.559 internal, 0.512 external), outperforming supervised and unsupervised baselines, and demonstrates improved radiologist sensitivity and reduced interpretation time in a reader study.
Significance. If the synthesized training data generalizes to real lesions, this annotation-free approach would be highly significant for prenatal imaging, where manual annotations for rare conditions like GMH-IVH are scarce and labor-intensive. The multi-site external validation, outperformance over baselines, and reader-study gains (sensitivity increase to 0.941-1.000 and 16-52.7% time reduction) provide concrete evidence of potential clinical utility for earlier diagnosis. The work's strength lies in its reproducible synthesis pipeline and falsifiable multi-center metrics, though moderate DSC values limit claims of precise localization.
major comments (1)
- [Methods (pseudo GMH-IVH synthesis)] Methods section on pseudo GMH-IVH image synthesis: The annotation-free claim is load-bearing on the assumption that synthesized images capture real GMH-IVH intensity profiles, textures, shapes, locations, and MRI artifacts across gestational ages and stages. No quantitative fidelity validation (intensity histograms, shape descriptors, or perceptual metrics) is reported. The external performance drop (sensitivity 0.914 to 0.824, DSC 0.559 to 0.512) and only moderate DSC indicate possible exploitation of synthesis-specific cues rather than true lesion features, leaving the domain-gap assumption untested and requiring empirical support such as an ablation study.
minor comments (1)
- [Abstract] Abstract and Results: The abstract states outperformance over baselines but does not quantify the margins or name the exact supervised/unsupervised methods; adding these details would improve clarity without altering the central claims.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback on our manuscript. We address the major comment on the pseudo-GMH-IVH synthesis validation below and will incorporate the suggested empirical support in the revised version.
read point-by-point responses
-
Referee: Methods section on pseudo GMH-IVH image synthesis: The annotation-free claim is load-bearing on the assumption that synthesized images capture real GMH-IVH intensity profiles, textures, shapes, locations, and MRI artifacts across gestational ages and stages. No quantitative fidelity validation (intensity histograms, shape descriptors, or perceptual metrics) is reported. The external performance drop (sensitivity 0.914 to 0.824, DSC 0.559 to 0.512) and only moderate DSC indicate possible exploitation of synthesis-specific cues rather than true lesion features, leaving the domain-gap assumption untested and requiring empirical support such as an ablation study.
Authors: We agree that quantitative fidelity metrics would strengthen the evidence that our synthesis captures real lesion characteristics. In the revision, we will add comparisons of intensity histograms, Haralick texture features, and shape descriptors (e.g., area, eccentricity) between synthesized and real GMH-IVH lesions drawn from the annotated validation cases. The observed external performance drop is expected given inter-site differences in scanner vendors, field strengths, and acquisition protocols; importantly, FreeHemoSeg still outperforms all supervised and unsupervised baselines on the external set, which would be unlikely if the model were merely exploiting synthesis-specific artifacts. We will further include an ablation study that systematically removes individual synthesis priors (intensity perturbation, location sampling, gestational-age scaling) and re-evaluates external generalization to isolate their contribution. These additions will directly test the domain-gap assumption. revision: yes
Circularity Check
No significant circularity in annotation-free training and validation pipeline
full rationale
The paper trains FreeHemoSeg exclusively on pseudo GMH-IVH images synthesized from normal fetal T2-weighted MRI using medical priors, then reports performance on independent real multi-site clinical cases (internal and external validation cohorts). No equations, derivations, or performance metrics reduce by construction to the synthesis inputs; the external-validation results (AUROC, sensitivity, DSC) are measured on held-out real data and thus constitute independent evidence. No load-bearing self-citations, uniqueness theorems, or ansatzes imported from prior author work are invoked to justify the central claim. The separation between synthetic training data and real evaluation data keeps the annotation-free assertion self-contained.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Medical priors can guide synthesis of realistic pseudo GMH-IVH images from normal fetal MRI data
Reference graph
Works this paper leans on
-
[1]
Fetal intracranial hemorrhage: role of fetal MRI: Fetal intracranial hemorrhage and fetal MRI
Sanapo L, Whitehead MT, Bulas DI, et al. Fetal intracranial hemorrhage: role of fetal MRI: Fetal intracranial hemorrhage and fetal MRI. Prenat Diagn. 2017;37(8):827–836. doi: 10.1002/pd.5096
-
[2]
Brouwer AJ, Groenendaal F, Benders MJNL, De Vries LS. Early and Late Complications of Germinal Matrix-Intraventricular Haemorrhage in the Preterm Infant: What Is New? Neonatology. 2014;106(4):296–303. doi: 10.1159/000365127
-
[3]
Hadi E, Haddad L, Levy M, et al. Fetal intraventricular hemorrhage and periventricular hemorrhagic venous infarction: time for dedicated classification system. Ultrasound Obstet Gynecol Off J Int Soc Ultrasound Obstet Gynecol. England; 2024;64(3):285–
work page 2024
-
[4]
doi: 10.1002/uog.27613
-
[5]
Fetal intracranial hemorrhage (fetal stroke): does grade matter? Ultrasound Obstet Gynecol
Elchalal U, Yagel S, Gomori JM, et al. Fetal intracranial hemorrhage (fetal stroke): does grade matter? Ultrasound Obstet Gynecol. 2005;26(3):233–243. doi: 10.1002/uog.1969
-
[6]
Antenatal diagnosis of fetal intraventricular hemorrhage: systematic review and meta‐analysis
Dunbar MJ, Woodward K, Leijser LM, Kirton A. Antenatal diagnosis of fetal intraventricular hemorrhage: systematic review and meta‐analysis. Dev Med Child Neurol. 2021;63(2):144–155. doi: 10.1111/dmcn.14713
-
[7]
Kim S, Jung YJ, Baik J, et al. Prenatal diagnosis and postnatal outcome of fetal intracranial hemorrhage: a single-center experience. Obstet Gynecol Sci. 2024;67(4):393–403. doi: 10.5468/ogs.24097
-
[8]
Epstein, Kline-Fath BM, Zhang B, et al
K.N. Epstein, Kline-Fath BM, Zhang B, et al. Prenatal Evaluation of Intracranial Hemorrhage on Fetal MRI: A Retrospective Review. Am J Neuroradiol. 2021;42(12):2222–2228. doi: 10.3174/ajnr.A7320
-
[9]
Moradi B, Ardestani RM, Shirazi M, Eslamian L, Kazemi MA. Fetal intracranial hemorrhage and infarct: Main sonographic and MRI characteristics: A review article. Eur J Obstet Gynecol Reprod Biol X. 2024;24:100351. doi: 10.1016/j.eurox.2024.100351
-
[10]
SmaRT: Style-Modulated Robust Test-Time Adaptation for Cross-Domain Brain Tumor Segmentation in MRI
Wang Y, Chen Y, Jiang S, et al. SmaRT: Style-Modulated Robust Test-Time Adaptation for Cross-Domain Brain Tumor Segmentation in MRI. ArXiv E-Prints. 2025;arXiv:2509.17925. doi: 10.48550/arXiv.2509.17925
-
[11]
Wang Y, Chen Y, Jiang S, et al. DR-TTA: Dynamic and Robust Test-Time Adaptation Under Low-Quality Mri Conditions for Brain Tumor Segmentation. 2025 IEEE Int Conf Bioinforma Biomed BIBM. 2025. p. 2899–2906. doi: 10.1109/BIBM66473.2025.11356381
-
[12]
Vggsound: A Large-Scale Audio-Visual Dataset
Huang H, Lin L, Tong R, et al. UNet 3+: A Full-Scale Connected UNet for Medical Image Segmentation. ICASSP 2020 - 2020 IEEE Int Conf Acoust Speech Signal Process ICASSP. Barcelona, Spain: IEEE; 2020. p. 1055–1059. doi: 10.1109/ICASSP40776.2020.9053405
-
[13]
H-denseunet: Hybrid densely connected unet for liver and tumor segmentation from ct volumes
Li X, Chen H, Qi X, Dou Q, Fu C-W, Heng P-A. H-DenseUNet: Hybrid Densely Connected UNet for Liver and Tumor Segmentation From CT Volumes. IEEE Trans Med Imaging. 2018;37(12):2663–2674. doi: 10.1109/TMI.2018.2845918
-
[14]
Low-grade intraventricular hemorrhage: is 16 ultrasound good enough? J Matern Fetal Neonatal Med
Alessandro Parodi AR Giovanni Morana, Maria S Severino, Mariya Malova, Anna R Natalizia, Andrea Sannia, Ramenghi LA. Low-grade intraventricular hemorrhage: is 16 ultrasound good enough? J Matern Fetal Neonatal Med. Taylor & Francis; 2015;28(sup1):2261–2264. doi: 10.3109/14767058.2013.796162
-
[15]
A Labeling-Free Approach to Supervising Deep Neural Networks for Retinal Blood Vessel Segmentation
Chen Y. A Labeling-Free Approach to Supervising Deep Neural Networks for Retinal Blood Vessel Segmentation. arXiv; 2017. http://arxiv.org/abs/1704.07502. Accessed August 19, 2024
-
[16]
Proxy-Bridged Image Reconstruction Network for Anomaly Detection in Medical Images
Zhou K, Li J, Luo W, et al. Proxy-Bridged Image Reconstruction Network for Anomaly Detection in Medical Images. IEEE Trans Med Imaging. 2022;41(3):582–594. doi: 10.1109/TMI.2021.3118223
-
[18]
Synthetic Data for Robust Stroke Segmentation
Chalcroft L, Pappas I, Price CJ, Ashburner J. Synthetic Data for Robust Stroke Segmentation. arXiv; 2024. http://arxiv.org/abs/2404.01946. Accessed August 19, 2024
-
[20]
Label-Free Segmentation of COVID-19 Lesions in Lung CT
Yao Q, Xiao L, Liu P, Zhou SK. Label-Free Segmentation of COVID-19 Lesions in Lung CT. IEEE Trans Med Imaging. 2021;40(10):2808–2819. doi: 10.1109/TMI.2021.3066161
-
[21]
LeFusion: Synthesizing Myocardial Pathology on Cardiac MRI via Lesion-Focus Diffusion Models
Zhang H, Yang J, Wan S, Fua P. LeFusion: Synthesizing Myocardial Pathology on Cardiac MRI via Lesion-Focus Diffusion Models. arXiv; 2024. http://arxiv.org/abs/2403.14066. Accessed August 19, 2024
-
[22]
Local Style Transfer via Latent Space Manipulation for Cross-Disease Lesion Segmentation
Lyu F, Ye M, Yip TC-F, Wong GL-H, Yuen PC. Local Style Transfer via Latent Space Manipulation for Cross-Disease Lesion Segmentation. IEEE J Biomed Health Inform. 2024;28(1):273–284. doi: 10.1109/JBHI.2023.3327726
-
[27]
Beyond Adapting SAM: Towards End-to-End Ultrasound Image Segmentation via Auto Prompting
Lin X, Xiang Y, Yu L, Yan Z. Beyond Adapting SAM: Towards End-to-End Ultrasound Image Segmentation via Auto Prompting. In: Linguraru MG, Dou Q, Feragen A, et al., editors. Med Image Comput Comput Assist Interv – MICCAI 2024. Cham: Springer Nature Switzerland; 2024. p. 24–34. 17
work page 2024
-
[31]
Lee W, Lee H, Lee H, Park EK, Nam H, Kooi T. Transformer-based Deep Neural Network for Breast Cancer Classification on Digital Breast Tomosynthesis Images. Radiol Artif Intell. 2023;5(3):e220159. doi: 10.1148/ryai.220159
-
[32]
Fetal Germinal Matrix and Intraventricular Hemorrhage
Morioka T, Hashiguchi K, Nagata S, et al. Fetal Germinal Matrix and Intraventricular Hemorrhage. Pediatr Neurosurg. 2006;42(6):354–361. doi: 10.1159/000095565
-
[33]
FETAL INTRAVENTRICULAR HAEMORRHAGE: DIFFERENT APPROACHES NEEDED? INSIGHTS ON GASLINI’S EXPERIENCE
Ramenghi LA, Samuele C. FETAL INTRAVENTRICULAR HAEMORRHAGE: DIFFERENT APPROACHES NEEDED? INSIGHTS ON GASLINI’S EXPERIENCE
-
[34]
Gonçalves LF, Lee W, Mody S, Shetty A, Sangi-Haghpeykar H, Romero R. Diagnostic accuracy of ultrasonography and magnetic resonance imaging for the detection of fetal anomalies: a blinded case-control study: Accuracy of US and MRI in detecting fetal anomalies. Ultrasound Obstet Gynecol. 2016;48(2):185–192. doi: 10.1002/uog.15774
-
[35]
Real-time automatic fetal brain extraction in fetal MRI by deep learning
Salehi SSM, Hashemi SR, Velasco-Annis C, et al. Real-time automatic fetal brain extraction in fetal MRI by deep learning. 2018 IEEE 15th Int Symp Biomed Imaging ISBI 2018. 2018. p. 720–724. doi: 10.1109/ISBI.2018.8363675
-
[36]
Prayer D, Malinger G, De Catte L, et al. ISUOG Practice Guidelines (updated): performance of fetal magnetic resonance imaging. Ultrasound Obstet Gynecol. 2023;61(2):278–287. doi: 10.1002/uog.26129. 18 Table 1. Baseline Characteristics of the Study Population Characteristic Training Dataset A Training Dataset B Validation Dataset A Validation Dataset B Fun...
-
[37]
Ebner M, Wang G, Li W, et al. An automated framework for localization, segmentation and super-resolution reconstruction of fetal brain MRI. NeuroImage. 2020;206:116324. doi: 10.1016/j.neuroimage.2019.116324
-
[38]
NeSVoR: Implicit Neural Representation for Slice-to- Volume Reconstruction in MRI
Xu J, Moyer D, Gagoski B, et al. NeSVoR: Implicit Neural Representation for Slice-to- Volume Reconstruction in MRI. IEEE Trans Med Imaging. 2023;42(6):1707–1719. doi: 10.1109/TMI.2023.3236216
-
[40]
A Dempster-Shafer approach to trustworthy AI with application to fetal brain MRI segmentation
Fidon L, Aertsen M, Kofler F, et al. A Dempster-Shafer approach to trustworthy AI with application to fetal brain MRI segmentation. IEEE Trans Pattern Anal Mach Intell. 2024;1–12. doi: 10.1109/TPAMI.2023.3346330
-
[41]
Papile L-A, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. Elsevier; 1978;92(4):529–534
work page 1978
-
[42]
https://doi.org/10.1007/978-3- 642-13875-1
Zhang Z, Deng H, Li X. Unsupervised Liver Tumor Segmentation with Pseudo Anomaly Synthesis. In: Wolterink JM, Svoboda D, Zhao C, Fernandez V, editors. Simul Synth Med Imaging. Cham: Springer Nature Switzerland; 2023. p. 86–96. doi: 10.1007/978-3- 031-44689-4_9
-
[43]
VM-UNet: Vision Mamba UNet for Medical Image Segmentation
Ruan J, Xiang S. VM-UNet: Vision Mamba UNet for Medical Image Segmentation. arXiv; 2024. http://arxiv.org/abs/2402.02491. Accessed August 19, 2024
-
[44]
https:// arxiv.org/abs/2401.10166
Liu Y, Tian Y, Zhao Y, et al. VMamba: Visual State Space Model. ArXiv. 2024;abs/2401.10166. https://api.semanticscholar.org/CorpusID:267035250
-
[45]
Decoupled weight decay regularization
Loshchilov I, Hutter F. Decoupled weight decay regularization. ArXiv Prepr ArXiv171105101. 2017
work page 2017
-
[46]
Kirillov A, Mintun E, Ravi N, et al. Segment anything. Proc IEEECVF Int Conf Comput Vis. 2023. p. 4015–4026
work page 2023
-
[47]
Beyond Adapting SAM: Towards End-to-End Ultrasound Image Segmentation via Auto Prompting
Lin X, Xiang Y, Yu L, Yan Z. Beyond Adapting SAM: Towards End-to-End Ultrasound Image Segmentation via Auto Prompting. In: Linguraru MG, Dou Q, Feragen A, et al., editors. Med Image Comput Comput Assist Interv – MICCAI 2024. Cham: Springer Nature Switzerland; 2024. p. 24–34
work page 2024
-
[48]
Adam: A method for stochastic optimization
Kingma DP. Adam: A method for stochastic optimization. ArXiv Prepr ArXiv14126980. 2014
work page 2014
-
[49]
Bias in Unsupervised Anomaly Detection in Brain MRI
Bercea CI, Puyol-Antón E, Wiestler B, Rueckert D, Schnabel JA, King AP. Bias in Unsupervised Anomaly Detection in Brain MRI. arXiv; 2023. http://arxiv.org/abs/2308.13861. Accessed August 29, 2023. 25
-
[50]
Liu M, Jiao Y, Lu J, Chen H. Anomaly Detection for Medical Images Using Teacher- Student Model with Skip Connections and Multi-scale Anomaly Consistency. IEEE Trans Instrum Meas. 2024;1–1. doi: 10.1109/TIM.2024.3406792
-
[51]
Informative knowledge distillation for image anomaly segmentation
Cao Y, Wan Q, Shen W, Gao L. Informative knowledge distillation for image anomaly segmentation. Knowl-Based Syst. 2022;248:108846. doi: 10.1016/j.knosys.2022.108846
-
[52]
Deng H, Li X. Anomaly Detection via Reverse Distillation from One-Class Embedding. 2022 IEEECVF Conf Comput Vis Pattern Recognit CVPR. New Orleans, LA, USA: IEEE; 2022. p. 9727–9736. doi: 10.1109/CVPR52688.2022.00951
-
[53]
Deep high-resolution representation learning for visual recognition
Wang J, Sun K, Cheng T, et al. Deep high-resolution representation learning for visual recognition. IEEE Trans Pattern Anal Mach Intell. IEEE; 2020;43(10):3349–3364
work page 2020
-
[54]
Zagoruyko S, Komodakis N. Wide Residual Networks. ArXiv Prepr ArXiv160507146. 2016
work page 2016
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.