Recognition: no theorem link
Diabetic Retinopathy Classification using Downscaling Algorithms and Deep Learning
Pith reviewed 2026-05-13 01:46 UTC · model grok-4.3
The pith
Downscaling algorithms with a multichannel Inception V3 network improve five-stage diabetic retinopathy classification on merged datasets.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The authors claim that applying downscaling algorithms to retinal images from the combined Kaggle and IDRiD datasets, followed by a self-crafted preprocessing phase and a Multi Channel Inception V3 architecture, produces higher accuracy, specificity, and sensitivity for five-class diabetic retinopathy classification than previous methods.
What carries the argument
Multi Channel Inception V3 architecture that receives downscaled images after custom preprocessing to perform five-stage severity classification.
If this is right
- The approach yields higher accuracy, specificity, and sensitivity than earlier state-of-the-art classifiers.
- Merging the Kaggle and IDRiD datasets creates a more representative training distribution for the five severity classes.
- Downscaling solves the problem of large and varying image sizes while maintaining classification quality.
- The pipeline supports reliable five-stage diabetic retinopathy labeling from fundus photographs.
Where Pith is reading between the lines
- Similar downscaling steps could reduce compute needs when applying deep networks to other high-resolution medical images.
- The method invites direct testing on retinopathy datasets collected from additional geographic populations.
- If external validation holds, the pipeline could raise detection rates in routine diabetic screening programs.
Load-bearing premise
The downscaling algorithms preserve clinically relevant features such as microaneurysms, hemorrhages, and exudates without introducing artifacts that would mislead the classifier.
What would settle it
Performance drop on a new external retinal image set where downscaled versions cause misclassification of early-stage cases containing visible microaneurysms.
Figures


read the original abstract
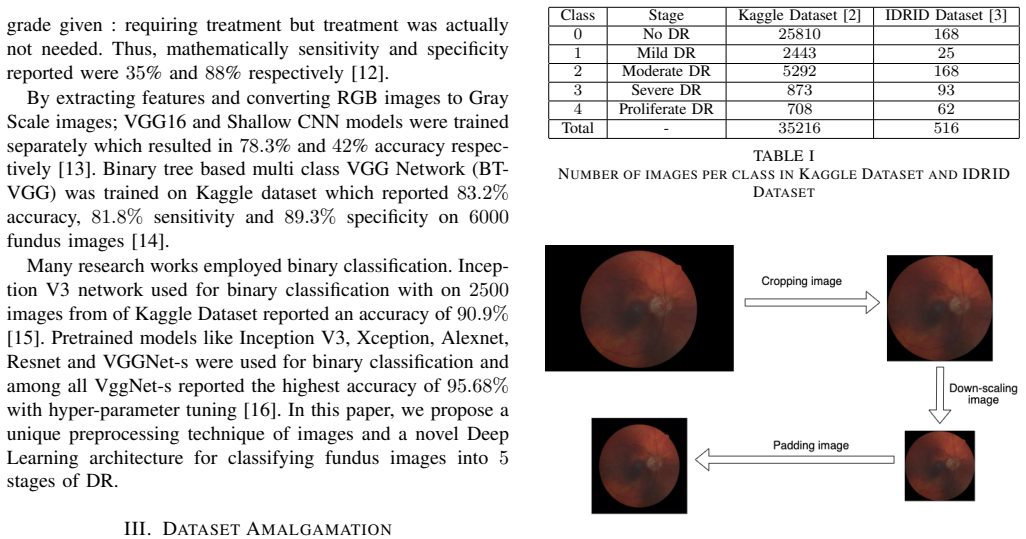
Diabetic Retinopathy (DR) is an art and science of recording and classifying the retinal images of a diabetic patient. DR classification deals with classifying retinal fundus image into five stages on the basis of severity of diabetes. One of the major issue faced while dealing with DR classification problem is the large and varying size of images. In this paper we propose and explore the use of several downscaling algorithms before feeding the image data to a Deep Learning Network for classification. For improving training and testing; we amalgamate two datasets: Kaggle and Indian Diabetic Retinopathy Image Dataset. Our experiments have been performed on a novel Multi Channel Inception V3 architecture with a unique self crafted preprocessing phase. We report results of proposed approach using accuracy, specificity and sensitivity, which outperform the previous state of the art methods. Index Terms: Diabetic Retinopathy, Downscaling Algorithms, Multichannel CNN Architecture, Deep Learning
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes applying several downscaling algorithms to high-resolution fundus images prior to classification with a novel multi-channel Inception-V3 architecture, after merging the Kaggle and IDRiD datasets and applying a self-crafted preprocessing phase. It claims that the resulting accuracy, sensitivity, and specificity outperform prior state-of-the-art methods for five-class diabetic retinopathy grading.
Significance. If the empirical claims were substantiated with reproducible numbers, ablations, and feature-preservation metrics, the work would address a practical bottleneck in retinal-image pipelines (input-size mismatch with standard CNNs) and could support more efficient automated DR screening. The dataset-merging strategy and multi-channel design are reasonable starting points, but the current manuscript supplies none of the required validation.
major comments (4)
- Abstract: the central claim that the proposed pipeline 'outperform[s] the previous state of the art methods' on accuracy, specificity, and sensitivity is unsupported by any numerical values, tables, baseline descriptions, train/test splits, or error bars, rendering the headline result unverifiable from the manuscript.
- Abstract and Methods: no description is given of the downscaling algorithms themselves, their parameters, or any quantitative check (e.g., expert-annotated lesion overlap or automated microaneurysm F1) that clinically relevant features survive the 5-10× reduction required for Inception-V3 input size.
- Experiments: the manuscript contains no ablation comparing the multi-channel model on native-resolution crops versus the downscaled inputs, so any reported gains cannot be attributed to the proposed downscaling step.
- Dataset section: the Kaggle+IDRiD merge is presented without domain-shift correction, label-consistency audit, or class-balance statistics, leaving open the possibility that performance differences arise from dataset artifacts rather than the method.
minor comments (2)
- Abstract: the sentence 'DR is an art and science of recording and classifying the retinal images' is imprecise and should be rephrased.
- Abstract: the phrase 'unique self crafted preprocessing phase' is undefined and should be replaced by an explicit list of steps.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed feedback. We address each major comment below and will revise the manuscript to strengthen the presentation of results, methods, and dataset details.
read point-by-point responses
-
Referee: Abstract: the central claim that the proposed pipeline 'outperform[s] the previous state of the art methods' on accuracy, specificity, and sensitivity is unsupported by any numerical values, tables, baseline descriptions, train/test splits, or error bars, rendering the headline result unverifiable from the manuscript.
Authors: We agree that the abstract would be strengthened by including concrete performance numbers. In the revised version we will add the reported accuracy, sensitivity, and specificity values, along with a concise reference to the baselines and dataset splits used, so that the central claim is immediately verifiable. revision: yes
-
Referee: Abstract and Methods: no description is given of the downscaling algorithms themselves, their parameters, or any quantitative check (e.g., expert-annotated lesion overlap or automated microaneurysm F1) that clinically relevant features survive the 5-10× reduction required for Inception-V3 input size.
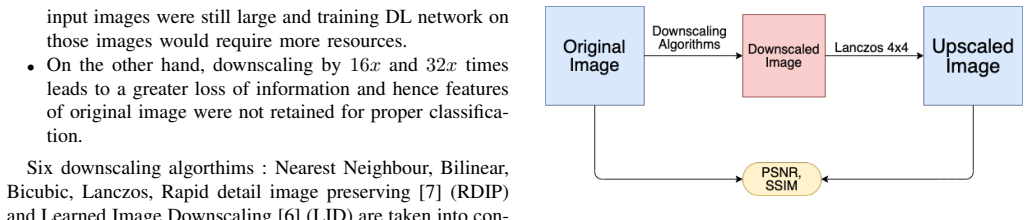
Authors: We appreciate this observation. The Methods section will be expanded to describe each downscaling algorithm (including bilinear, bicubic, and nearest-neighbor variants) and their exact parameters. We will also add quantitative feature-preservation metrics such as PSNR, SSIM, and microaneurysm detection F1 scores computed on expert-annotated regions to demonstrate that clinically relevant lesions are retained after downscaling. revision: yes
-
Referee: Experiments: the manuscript contains no ablation comparing the multi-channel model on native-resolution crops versus the downscaled inputs, so any reported gains cannot be attributed to the proposed downscaling step.
Authors: This is a fair criticism. We will include a new ablation study that directly compares the multi-channel Inception-V3 trained on native-resolution crops (with appropriate padding or cropping to meet input-size constraints) against the same architecture trained on the downscaled images. This will allow readers to attribute performance differences to the downscaling step. revision: yes
-
Referee: Dataset section: the Kaggle+IDRiD merge is presented without domain-shift correction, label-consistency audit, or class-balance statistics, leaving open the possibility that performance differences arise from dataset artifacts rather than the method.
Authors: We agree that greater transparency is required. The revised Dataset section will report class-balance statistics for the merged collection, describe the label-consistency checks performed across the two sources, and discuss observed domain differences together with the preprocessing steps used to reduce their impact. revision: yes
Circularity Check
No circularity: purely empirical pipeline with no derivation chain
full rationale
The paper presents an experimental workflow: downscaling fundus images, merging Kaggle and IDRiD datasets, training a multi-channel Inception-V3 model, and reporting accuracy/sensitivity/specificity. No equations, derivations, or parameter-fitting steps are described that could reduce to self-definition or fitted inputs renamed as predictions. All claims rest on direct empirical measurement rather than any load-bearing self-citation or ansatz. This matches the default expectation for non-circular empirical ML papers.
Axiom & Free-Parameter Ledger
free parameters (2)
- downscaling algorithm parameters
- network hyperparameters
axioms (2)
- domain assumption Downscaled retinal images retain sufficient diagnostic features for five-class severity grading.
- domain assumption The amalgamated Kaggle and IDRiD datasets form a single coherent distribution without harmful domain shift.
Reference graph
Works this paper leans on
-
[1]
Automated detection of diabetic retinopathy using deep learning,
C. Lam, D. Yi, M. Guo, and T. Lindsey, “Automated detection of diabetic retinopathy using deep learning,”AMIA Joint Summits on Translational Science proceedings. AMIA Joint Summits on Translational Science, vol. 2017, pp. 147–155, 05 2018
work page 2017
-
[2]
Diabetic retinopathy detection,
Kaggle Inc., “Diabetic retinopathy detection,” 2015, kaggle competition dataset. [Online]. Available: https://www.kaggle.com/c/diabetic- retinopathy-detection
work page 2015
-
[3]
Indian diabetic retinopathy image dataset (IDRiD),
P. Porwal, S. Pachade, R. Kamble, M. Kokare, G. Deshmukh, V . Sahasrabuddhe, and F. Meriaudeau, “Indian diabetic retinopathy image dataset (IDRiD),” 2018, iEEE DataPort dataset. [Online]. Available: http://dx.doi.org/10.21227/H25W98
-
[4]
A comparative analysis of image interpo- lation algorithms,
P. Parsania and D. Virparia, “A comparative analysis of image interpo- lation algorithms,”IJARCCE, vol. 5, pp. 29–34, 01 2016
work page 2016
-
[5]
Image interpolation techniques in digital image processing: An overview,
S. Fadnavis, “Image interpolation techniques in digital image processing: An overview,”International Journal Of Engineering Research and Application, vol. 4, pp. 2248–962 270, 11 2014
work page 2014
-
[6]
Learned image downscaling for upscaling using content adaptive resampler,
W. Sun and Z. Chen, “Learned image downscaling for upscaling using content adaptive resampler,”IEEE Transactions on Image Processing, vol. 29, pp. 4027 – 4040, 02 2020
work page 2020
-
[7]
N. Weber, M. Waechter, S. C. Amend, S. Guthe, and M. Goesele, “Rapid, detail-preserving image downscaling,”ACM Trans. Graph., vol. 35, no. 6, pp. 205:1–205:6, Nov. 2016. [Online]. Available: http://doi.acm.org/10.1145/2980179.2980239
-
[8]
Application of higher order spectra for the identification of diabetes retinopathy stages,
R. Acharya U, C. K. Chua, E. Y . Ng, W. Yu, and C. Chee, “Application of higher order spectra for the identification of diabetes retinopathy stages,”J. Med. Syst., vol. 32, no. 6, p. 481–488, Dec. 2008. [Online]. Available: https://doi.org/10.1007/s10916-008-9154-8
-
[9]
Automated detection of dia- betic retinopathy using SVM,
E. Carrera, A. Gonz ´alez, and R. Carrera, “Automated detection of dia- betic retinopathy using SVM,” in2017 IEEE International Conference on Interdisciplinary Research (INTERCON), 08 2017, pp. 1–6
work page 2017
-
[10]
O. Faust, U. R. Acharya, E. Ng, N. Kh, and J. Suri, “Algorithms for the automated detection of diabetic retinopathy using digital fundus images: A review,”Journal of medical systems, vol. 36, pp. 145–57, 02 2012
work page 2012
-
[11]
Convo- lutional neural networks for diabetic retinopathy,
H. Pratt, F. Coenen, D. Broadbent, S. Harding, and Y . Zheng, “Convo- lutional neural networks for diabetic retinopathy,”Procedia Computer Science, vol. 90, pp. 200–205, 12 2016
work page 2016
-
[12]
H. Takahashi, H. Tampo, Y . Arai, Y . Inoue, and H. Kawashima, “Apply- ing artificial intelligence to disease staging: Deep learning for improved staging of diabetic retinopathy,”PLOS ONE, vol. 12, p. e0179790, 06 2017
work page 2017
-
[13]
Classification of diabetic retinopathy images by using deep learning models,
S. Dutta, B. Manideep, M. Basha, R. Caytiles, and N. C. S. N. Iyenger, “Classification of diabetic retinopathy images by using deep learning models,”International Journal of Grid and Distributed Computing, vol. 11, pp. 89–106, 01 2018
work page 2018
-
[14]
On the grading of diabetic retinopathies using a binary-tree-based multiclass classifier of cnns,
M. M. Adly, A. S. Ghoneim, and A. A. Youssif, “On the grading of diabetic retinopathies using a binary-tree-based multiclass classifier of cnns,”International Journal of Computer Science and Information Security (IJCSIS), vol. 17, 01 2019
work page 2019
-
[15]
Transfer learning based detection of diabetic retinopathy from small dataset,
M. T. Hagos and S. Kant, “Transfer learning based detection of diabetic retinopathy from small dataset,” Online preprint, 05 2019
work page 2019
-
[16]
Deep convolutional neural networks for diabetic retinopathy detection by image classification,
S. Wan, Y . Liang, and Y . Zhang, “Deep convolutional neural networks for diabetic retinopathy detection by image classification,”Computers & Electrical Engineering, vol. 72, pp. 274–282, 11 2018
work page 2018
-
[17]
Communication in the presence of noise,
C. E. Shannon, “Communication in the presence of noise,”Proc. Institute of Radio Engineers, vol. 37, no. 1, pp. 10–21, 1949
work page 1949
-
[18]
Comparison of image quality assessment: Psnr, hvs, ssim, uiqi,
Y . Al-Najjar and S. D. Chen, “Comparison of image quality assessment: Psnr, hvs, ssim, uiqi,”International Journal of Scientific & Engineering Research, vol. 3, pp. 1–5, 01 2012
work page 2012
-
[19]
ImageNet: A large-scale hierarchical image database,
J. Deng, W. Dong, R. Socher, L.-J. Li, K. Li, and F. F. Li, “ImageNet: A large-scale hierarchical image database,” inProc. IEEE Conf. Computer Vision and Pattern Recognition (CVPR), 06 2009, pp. 248–255
work page 2009
-
[20]
Rethinking the Inception Architecture for Computer Vision
C. Szegedy, V . Vanhoucke, S. Ioffe, J. Shlens, and Z. Wojna, “Rethinking the inception architecture for computer vision,”CoRR, vol. abs/1512.00567, 2015. [Online]. Available: http://arxiv.org/abs/1512.00567
work page Pith review arXiv 2015
-
[21]
Diagnostic methods i: Sensitivity, specificity, and other measures of accuracy,
K. Stralen, V . Stel, J. Reitsma, F. Dekker, C. Zoccali, and K. Jager, “Diagnostic methods i: Sensitivity, specificity, and other measures of accuracy,”Kidney international, vol. 75, pp. 1257–63, 05 2009
work page 2009
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.