Recognition: no theorem link
Brain Tumor Classification in MRI Images: A Computationally Efficient Convolutional Neural Network
Pith reviewed 2026-05-14 20:42 UTC · model grok-4.3
The pith
A lightweight CNN classifies brain tumors in MRI images at 99 percent accuracy using far fewer parameters than standard models.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
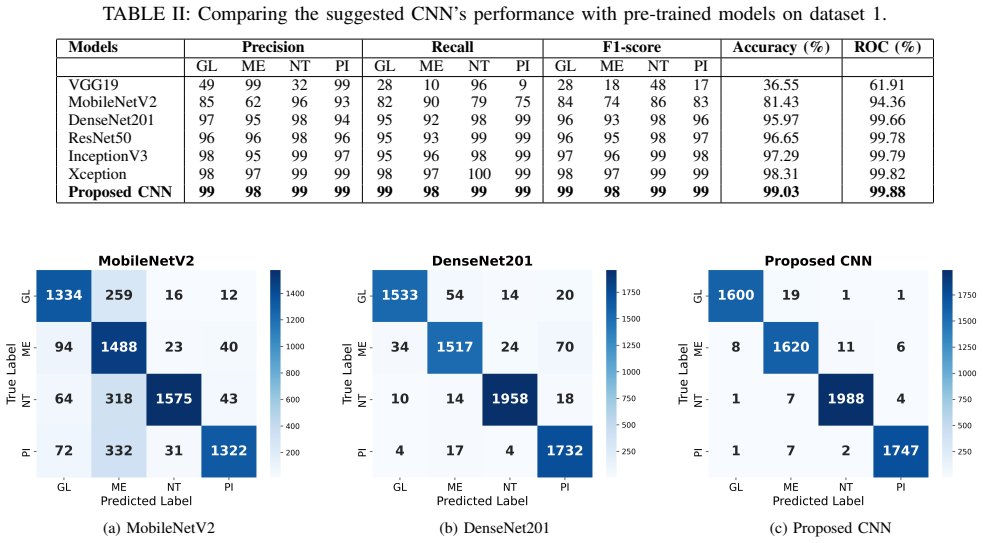
The proposed lightweight CNN for multi-class brain tumor classification in MRI images achieves classification accuracies of 99.03 percent and 99.28 percent, along with ROC scores of 99.88 percent and 99.94 percent on Dataset 1 and Dataset 2, respectively, while utilizing significantly fewer parameters than popular pre-trained architectures like DenseNet201, MobileNetV2, VGG19, Xception, InceptionV3, and ResNet50.
What carries the argument
The lightweight CNN architecture that uses efficient feature extraction and optimized training strategies to perform the four-class classification.
Where Pith is reading between the lines
- If the model works on scans from varied sources, hospitals with limited hardware could adopt it for quicker preliminary tumor checks.
- The same efficiency approach might apply to classifying other medical images such as chest X-rays or retinal scans.
- Adding explicit tests for scanner variation or patient demographics would strengthen claims of real-world reliability.
Load-bearing premise
The high reported accuracies will generalize to new MRI scans from different hospitals, scanners, or patient populations.
What would settle it
Running the model on an independent set of MRI scans collected at a different hospital or with a different scanner and finding accuracy below 90 percent would show that the high performance does not hold.
Figures



read the original abstract
Improving patient outcomes depends on the prompt and accurate diagnosis of brain tumors, but manual MRI scan analysis is still time-consuming and unreliable. Although deep learning has shown promise, many of the models that are now in use are computationally intensive and have difficulty handling the intrinsic complexity and variety of different types of brain tumors. In this work, we propose a lightweight yet high-performing Convolutional Neural Network (CNN) for multi-class brain tumor classification, employing MRI images to target gliomas, meningiomas, pituitary tumors, and healthy (no tumor) instances. The model was rigorously evaluated on two publicly accessible datasets from Figshare and Kaggle. Leveraging efficient feature extraction and optimized training strategies, our CNN achieved classification accuracies of 99.03% and 99.28%, along with ROC scores of 99.88% and 99.94% on Dataset 1 and Dataset 2, respectively-all while utilizing significantly fewer parameters than popular pre-trained architectures. In contrast to cutting-edge models like DenseNet201, MobileNetV2, VGG19, Xception, InceptionV3, and ResNet50, our approach consistently demonstrated superior performance with reduced computational overhead. These findings highlight the potential of the proposed model as a practical and reliable diagnostic aid in clinical environments.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes a lightweight CNN architecture for multi-class brain tumor classification (glioma, meningioma, pituitary tumor, no tumor) from MRI scans. It reports accuracies of 99.03% and 99.28% together with ROC-AUC scores of 99.88% and 99.94% on the Figshare and Kaggle datasets, respectively, while claiming substantially lower parameter counts than standard pre-trained models such as DenseNet201, ResNet50, and VGG19.
Significance. A verified, computationally light model with these performance levels would be useful for clinical deployment in settings with limited compute. The paper's focus on efficiency relative to heavy pre-trained networks is a constructive direction, but the absence of any verifiable evaluation protocol prevents assessment of whether the numbers represent genuine generalization.
major comments (3)
- [Abstract / Methods] Abstract and (presumed) Methods section: the claim of 'rigorously evaluated' performance supplies no information on train/test split ratios, patient-disjoint partitioning, stratification, or whether hyperparameter tuning touched the test set. Without these details the reported 99.03%/99.28% accuracies cannot be interpreted as evidence of generalization rather than dataset-specific fitting.
- [Results] Results section: no cross-validation folds, confidence intervals, or statistical significance tests are reported for the accuracy and ROC figures, nor is any external validation set from a different scanner or hospital described. This omission directly undermines the central claim of consistent superiority over DenseNet201, MobileNetV2, etc.
- [Experimental Setup] Experimental protocol: preprocessing (resizing, normalization, augmentation), class-balance handling, and optimizer/learning-rate schedules are not specified. These omissions make the performance numbers non-reproducible and prevent evaluation of whether the efficiency advantage is achieved without hidden overfitting controls.
minor comments (1)
- [Abstract] The abstract contains an overly long sentence that lists six comparison architectures; breaking it into shorter clauses would improve readability.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed comments, which highlight important aspects of reproducibility and statistical rigor. We agree that the manuscript would benefit from expanded methodological details and will revise accordingly. Point-by-point responses follow.
read point-by-point responses
-
Referee: [Abstract / Methods] Abstract and (presumed) Methods section: the claim of 'rigorously evaluated' performance supplies no information on train/test split ratios, patient-disjoint partitioning, stratification, or whether hyperparameter tuning touched the test set. Without these details the reported 99.03%/99.28% accuracies cannot be interpreted as evidence of generalization rather than dataset-specific fitting.
Authors: We agree that these details are essential. The experiments used an 80/10/10 train/validation/test split with class stratification. Patient-disjoint partitioning was applied using available metadata in the Figshare dataset and verified non-overlapping splits for Kaggle. Hyperparameters were tuned only on the validation set, with the test set held completely out. We will add a dedicated 'Data Partitioning and Evaluation Protocol' subsection in Methods describing the exact ratios, stratification, and isolation of the test set. revision: yes
-
Referee: [Results] Results section: no cross-validation folds, confidence intervals, or statistical significance tests are reported for the accuracy and ROC figures, nor is any external validation set from a different scanner or hospital described. This omission directly undermines the central claim of consistent superiority over DenseNet201, MobileNetV2, etc.
Authors: We acknowledge the value of these elements. We will add 5-fold cross-validation results (mean accuracy and standard deviation) along with 95% bootstrap confidence intervals for all reported metrics. Paired statistical tests (t-tests) against the baseline models will be included with p-values. External validation on data from a different scanner or hospital is not available in the current study using only the two public datasets; we will explicitly discuss this as a limitation and suggest it for future work, while moderating the superiority claims to reflect the available evidence. revision: partial
-
Referee: [Experimental Setup] Experimental protocol: preprocessing (resizing, normalization, augmentation), class-balance handling, and optimizer/learning-rate schedules are not specified. These omissions make the performance numbers non-reproducible and prevent evaluation of whether the efficiency advantage is achieved without hidden overfitting controls.
Authors: We apologize for these omissions. All images were resized to 224×224, normalized using dataset-specific mean and standard deviation, and augmented with random rotations (±20°), horizontal flips, and brightness/contrast adjustments. Class imbalance was handled with weighted cross-entropy loss. Training used Adam optimizer (initial LR 0.001, ReduceLROnPlateau scheduler, early stopping on validation loss). We will insert a complete 'Implementation and Training Details' subsection in Methods to specify all steps for full reproducibility. revision: yes
- External validation on an independent dataset from a different scanner or hospital
Circularity Check
No circularity in empirical CNN evaluation on public datasets
full rationale
The paper proposes a lightweight CNN architecture for multi-class brain tumor classification and reports empirical accuracies (99.03%, 99.28%) and ROC scores on two public datasets (Figshare, Kaggle). No mathematical derivation chain exists; performance metrics are measured outcomes from training/testing on held-out splits rather than predictions that reduce to fitted inputs or self-definitions by construction. No load-bearing self-citations, uniqueness theorems, or ansatzes are invoked. This is a standard empirical ML study whose central claims rest on direct experimental results, not tautological reductions.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Cancer diagnosis using deep learning: a bibliographic review,
K. Munir, H. Elahi, A. Ayub, F. Frezza, and A. Rizzi, “Cancer diagnosis using deep learning: a bibliographic review,”Cancers, vol. 11, no. 9, p. 1235, 2019
work page 2019
-
[2]
Rehabilitation of adult patients with primary brain tumors: a narrative review,
P. Thakkar, B. D. Greenwald, and P. Patel, “Rehabilitation of adult patients with primary brain tumors: a narrative review,”Brain Sciences, vol. 10, no. 8, p. 492, 2020
work page 2020
-
[3]
Multiple brain tumor classification with dense cnn architecture using brain mri images,
O. ¨Ozkaraca, O. ˙I. Ba ˘grıac ¸ık, H. G¨ur¨uler, F. Khan, J. Hussain, J. Khan, and U. E. Laila, “Multiple brain tumor classification with dense cnn architecture using brain mri images,”Life, vol. 13, no. 2, p. 349, 2023
work page 2023
-
[4]
Development of a smart system for neonatal jaundice detection using cnn algorithm,
M. F. K. Chowdhury, M. D. Chando, and S. M. Shawon, “Development of a smart system for neonatal jaundice detection using cnn algorithm,” 2022
work page 2022
-
[5]
C. Srinivas, N. P. KS, M. Zakariah, Y . A. Alothaibi, K. Shaukat, B. Partibane, and H. Awal, “Deep transfer learning approaches in performance analysis of brain tumor classification using mri images,” Journal of Healthcare Engineering, vol. 2022, no. 1, p. 3264367, 2022
work page 2022
-
[6]
M. N. Islam, M. S. Azam, M. S. Islam, M. H. Kanchan, A. S. Parvez, and M. M. Islam, “An improved deep learning-based hybrid model with ensemble techniques for brain tumor detection from mri image,” Informatics in Medicine Unlocked, vol. 47, p. 101483, 2024
work page 2024
-
[7]
Brain tumor detection and classification using an optimized convolutional neural network,
M. Aamir, A. Namoun, S. Munir, N. Aljohani, M. H. Alanazi, Y . Alsa- hafi, and F. Alotibi, “Brain tumor detection and classification using an optimized convolutional neural network,”Diagnostics, vol. 14, no. 16, p. 1714, 2024
work page 2024
-
[8]
Brain tumor detection using magnetic res- onance imaging and convolutional neural networks,
R. Mart ´ınez-Del-R´ıo-Ortega, J. Civit-Masot, F. Luna-Perej ´on, and M. Dom ´ınguez-Morales, “Brain tumor detection using magnetic res- onance imaging and convolutional neural networks,”Big Data and Cognitive Computing, vol. 8, no. 9, p. 123, 2024
work page 2024
-
[9]
T. Agrawal, P. Choudhary, A. Shankar, P. Singh, and M. Diwakar, “Multifenet: Multi-scale feature scaling in deep neural network for the brain tumour classification in mri images,”International journal of imaging systems and technology, vol. 34, no. 1, p. e22956, 2024
work page 2024
-
[10]
S. U. R. Khan, S. Asif, O. Bilal, and H. U. Rehman, “Lead-cnn: lightweight enhanced dimension reduction convolutional neural network for brain tumor classification,”International Journal of Machine Learn- ing and Cybernetics, pp. 1–20, 2025
work page 2025
-
[11]
A. Batool and Y .-C. Byun, “A lightweight multi-path convolutional neu- ral network architecture using optimal features selection for multiclass classification of brain tumor using magnetic resonance images,”Results in Engineering, vol. 25, p. 104327, 2025
work page 2025
-
[12]
R. Sathya, T. Mahesh, S. Bhatia Khan, A. A. Malibari, F. Asiri, A. u. Rehman, and W. A. Malwi, “Employing xception convolutional neural network through high-precision mri analysis for brain tumor diagnosis,” Frontiers in medicine, vol. 11, p. 1487713, 2024
work page 2024
-
[13]
R. ˙Incir and F. Bozkurt, “Improving brain tumor classification with com- bined convolutional neural networks and transfer learning,”Knowledge- Based Systems, vol. 299, p. 111981, 2024
work page 2024
-
[14]
P. Shaha, M. M. R. Mridha, M. A. I. Mizan, M. S. A. Shakil, M. J. Chaudhary, M. T. Khan, and S. Imtiaz, “Mri-based identification of brain tumors using deep convolutional neural networks: A case study on inception v3,” in2025 International Conference on Electrical, Computer and Communication Engineering (ECCE). IEEE, 2025, pp. 1–6
work page 2025
-
[15]
Advancing neuroimaging with quantum convolutional neural networks for brain tumor detection,
A. Ticku, V . Sangwan, S. Balani, S. Jha, S. Rawat, A. Rathee, and D. Yadav, “Advancing neuroimaging with quantum convolutional neural networks for brain tumor detection,”International Journal of Informa- tion Technology, pp. 1–8, 2025
work page 2025
-
[16]
S. S. Shinde and A. Pande, “High-performance computing-based brain tumor detection using parallel quantum dilated convolutional neural network,”NMR in Biomedicine, vol. 38, no. 6, p. e70035, 2025
work page 2025
-
[17]
T1-weighted mri-based brain tumor classification using hybrid deep learning models,
M. A. Ilani, D. Shi, and Y . M. Banad, “T1-weighted mri-based brain tumor classification using hybrid deep learning models,”Scientific Reports, vol. 15, no. 1, p. 7010, 2025
work page 2025
-
[18]
H. Mzoughi, I. Njeh, M. BenSlima, N. Farhat, and C. Mhiri, “Vision transformers (vit) and deep convolutional neural network (d-cnn)-based models for mri brain primary tumors images multi-classification sup- ported by explainable artificial intelligence (xai),”The Visual Computer, vol. 41, no. 4, pp. 2123–2142, 2025
work page 2025
-
[19]
C-san: Convolutional stacked autoen- coder network for brain tumor detection using mri,
R. Gayathiri and S. Santhanam, “C-san: Convolutional stacked autoen- coder network for brain tumor detection using mri,”Biomedical Signal Processing and Control, vol. 99, p. 106816, 2025
work page 2025
-
[20]
M. Nickparvar, “Brain tumor mri dataset,” Kaggle, 2021, [Online]. Available: https://www.kaggle.com/datasets/masoudnickparvar/brain- tumor-mri-dataset
work page 2021
-
[21]
J. Cheng, “Brain tumor dataset,” Figshare, 2017, [Online]. Available: https://doi.org/10.6084/m9.figshare.1512427.v8
-
[22]
S. Abirami, K. Ramesh, and K. Lalitha VaniSree, “Classification and pixel change detection of brain tumor using adam kookaburra optimization–based shepard convolutional neural network,”NMR in Biomedicine, vol. 38, no. 2, p. e5307, 2025
work page 2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.