Cross-Modal Contrastive Learning of ECG and Angiography Representations for Severe Stenosis Classification
Pith reviewed 2026-06-30 13:49 UTC · model grok-4.3
The pith
Cross-modal contrastive pretraining on paired ECG and angiography data lets ECG models classify severe coronary stenosis at high accuracy.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
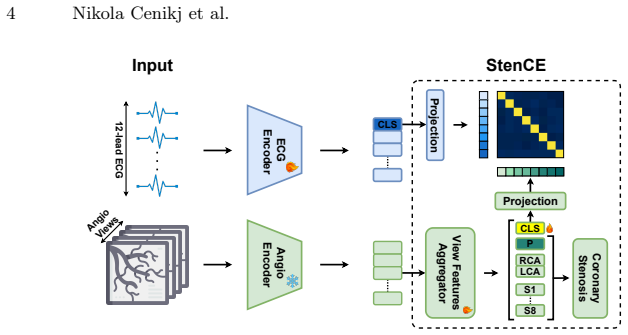
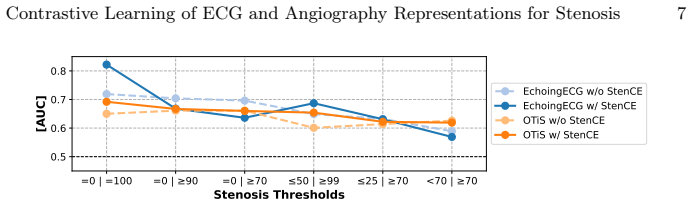
By applying cross-modal contrastive learning between ECG and angiography representations, the StenCE framework produces ECG encoders that extract stenosis-specific features, enabling accurate classification of severe coronary artery stenosis from ECG alone and outperforming earlier approaches on multiple severity thresholds and auxiliary ECG tasks.
What carries the argument
StenCE pretraining framework, which performs contrastive alignment of ECG and angiography representations to transfer stenosis signals into an ECG-only encoder.
If this is right
- ECG-based risk stratification becomes feasible for asymptomatic patients who would not otherwise receive angiography.
- The same pretrained encoders improve performance on other ECG classification tasks beyond stenosis.
- Performance remains stable across different choices of stenosis severity threshold.
- Only routine ECG acquisition is needed at inference time after pretraining.
Where Pith is reading between the lines
- If the learned signal generalizes across hospitals, ECG screening protocols could shift to include automated stenosis alerts for broader populations.
- The approach opens the possibility of combining the ECG encoder with other non-invasive signals such as blood pressure or symptoms for multi-modal triage.
- Retraining the contrastive step on larger paired datasets could further improve the specificity of the extracted ECG features.
Load-bearing premise
The alignment step extracts a genuine stenosis signal that exists in the ECG rather than dataset-specific correlations tied to the angiography labels.
What would settle it
Measure classification performance on an external ECG dataset collected at a different site where angiography ground truth is available but the contrastive pairs were never seen during training.
Figures

read the original abstract
Coronary artery stenosis is a common cardiovascular disease, with severe, untreated cases posing significant risks of heart attack. Although coronary (X-ray) angiograms remain the standard for stenosis diagnosis, they are invasive, time- and resource-intensive, and therefore only performed on patients with a high probability of disease based on symptoms and prior clinical tests. However, a subset of patients, especially those without symptoms, may remain undiagnosed. Detecting indications of stenosis from ECGs, which are fast, cheap, non-invasive, and thus routinely acquired even in asymptomatic patients, would support early diagnosis. However, as no reliable stenosis-specific signal has been identified in ECGs, they can not currently be used for stenosis risk stratification. To address this, we introduce StenCE, a pretraining framework, allowing stratification of patients based on features derived directly from ECGs. Evaluations across varying stenosis severity thresholds and additional ECG disease classification tasks demonstrate consistent performance improvements across different ECG encoders, outperforming previous work. The obtained models successfully detect signals for stenosis diagnosis in ECGs and are the first to achieve high performance in severe stenosis classification. The source code is available at https://github.com/NikolaCenic/ecg-stenosis-cls.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces StenCE, a cross-modal contrastive pretraining framework that aligns ECG and angiography representations to enable severe stenosis classification from ECG input alone. It reports consistent performance gains across multiple ECG encoders and tasks (including varying stenosis severity thresholds and other ECG disease classifications), outperforming prior work, and claims to be the first to achieve high performance in severe stenosis classification from ECGs. Source code is released.
Significance. If the central claim holds, the result would be significant for enabling non-invasive, routine ECG-based risk stratification for coronary stenosis in asymptomatic patients where angiography is not indicated. The open-source code release is a clear strength that supports reproducibility and follow-up work.
major comments (2)
- [Abstract] Abstract and evaluation description: the claim of 'consistent performance improvements' and 'high performance in severe stenosis classification' is load-bearing for the central contribution, yet the provided text supplies no dataset size, exclusion criteria, performance metrics (AUC/accuracy/F1), statistical tests, or ablation results. This prevents verification that gains arise from the contrastive mechanism rather than label recovery or dataset artifacts.
- [Method] Method and evaluation sections: the contrastive objective uses angiography-derived labels as the supervision signal for the downstream ECG-only task. Without an explicit comparison to a purely supervised ECG baseline trained on the identical labels (or controls for site/patient-selection biases), the attribution that the alignment 'extracts a stenosis-specific signal' present in the ECG waveform remains unverified and is central to the paper's mechanistic claim.
minor comments (2)
- [Introduction] The statement that 'no reliable stenosis-specific signal has been identified in ECGs' would benefit from additional citations to prior ECG-based attempts at stenosis detection to contextualize the novelty.
- [Method] Notation for the contrastive loss and the definition of positive/negative pairs should be clarified with an equation or pseudocode for readers unfamiliar with the specific alignment strategy.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive comments. We address each major point below and are prepared to revise the manuscript to strengthen the presentation and verification of our claims.
read point-by-point responses
-
Referee: [Abstract] Abstract and evaluation description: the claim of 'consistent performance improvements' and 'high performance in severe stenosis classification' is load-bearing for the central contribution, yet the provided text supplies no dataset size, exclusion criteria, performance metrics (AUC/accuracy/F1), statistical tests, or ablation results. This prevents verification that gains arise from the contrastive mechanism rather than label recovery or dataset artifacts.
Authors: We agree that the abstract is concise and omits numerical details. The full manuscript reports dataset characteristics, exclusion criteria, and performance metrics (including AUC, accuracy, and F1) with statistical tests in the Experiments and Results sections, along with ablation studies comparing pretraining variants. To address the concern directly, we will expand the abstract to include key dataset size, main performance numbers, and a brief note on ablations. These ablations isolate the contribution of the cross-modal contrastive objective beyond label supervision alone. revision: yes
-
Referee: [Method] Method and evaluation sections: the contrastive objective uses angiography-derived labels as the supervision signal for the downstream ECG-only task. Without an explicit comparison to a purely supervised ECG baseline trained on the identical labels (or controls for site/patient-selection biases), the attribution that the alignment 'extracts a stenosis-specific signal' present in the ECG waveform remains unverified and is central to the paper's mechanistic claim.
Authors: We recognize that a direct supervised baseline comparison is necessary to isolate the effect of cross-modal alignment. In the revised version we will add results for an ECG-only supervised model trained end-to-end on the identical angiography-derived stenosis labels using the same data splits, encoders, and evaluation protocol. We will also explicitly discuss dataset curation steps taken to mitigate site and selection biases and report any additional controls. revision: yes
Circularity Check
No significant circularity; empirical method relies on external paired data
full rationale
The paper introduces a contrastive pretraining framework (StenCE) that aligns ECG and angiography representations from paired external data, then evaluates downstream ECG-only classification performance on stenosis labels. No equations, derivations, or self-referential steps are described that reduce any prediction or result to its inputs by construction. The approach does not fit target labels directly during pretraining, invoke self-citations for uniqueness theorems, or rename known results. Performance claims are empirical and testable against independent benchmarks, making the derivation chain self-contained with no load-bearing reductions to the paper's own fitted values or definitions.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
- [1]
-
[2]
C. Cong, Y. Kato, H. D. Vasconcellos, M. Ostovaneh, J. Lima, and B. Ambale- Venkatesh: Deep learning-based end-to-end automated stenosis classification and localization on catheter coronary angiography. Frontiers in Cardiovascular Medicine10, 944135 (02 2023).https://doi.org/10.3389/fcvm.2023.944135
-
[3]
https://doi.org/10.48550/arXiv.2602.02067
Cenikj, N., Özgün Turgut, Müller, A., Steger, A., Kehrer, J., Brugger, M., Rueck- ert, D., Martens, E., Müller, P.: Multi-view stenosis classification leveraging transformer-based multiple-instance learning using real-world clinical data (2026). https://doi.org/10.48550/arXiv.2602.02067
-
[4]
https://doi.org/10.48550/arXiv.2503.15940
Chen, Y., Du, C., Li, C., Hu, J., Shi, Y., Xiong, S., Zhu, X.X., Mou, L.: Uni- crossadapter: Multimodal adaptation of clip for radiology report generation (2025). https://doi.org/10.48550/arXiv.2503.15940
-
[5]
Annals of Internal Medicine89(1), 1–5 (1978)
Crawford, M.H., Mendoza, C.A., O’Rourke, R.A., White, D.H., Boucher, C.A., , Gorwit, J.: Limitations of continuous ambulatory electrocardiogram monitoring for detecting coronary artery disease. Annals of Internal Medicine89(1), 1–5 (1978). https://doi.org/10.7326/0003-4819-89-1-1, pMID: 666154
-
[6]
D. L. Rodrigues, M. N. Menezes, F. J. Pinto, and A. L. Oliveira: Automated Detection of Coronary Artery Stenosis in X-ray Angiography using Deep Neural Networks (2021).https://doi.org/10.48550/arXiv.2103.02969
-
[7]
13026/3ykd-bf14, version 1.1.0
Elias, P., Finer, J.: EchoNext: A Dataset for Detecting Echocardiogram-Confirmed StructuralHeartDiseasefromECGs.PhysioNet(Sep2025).https://doi.org/10. 13026/3ykd-bf14, version 1.1.0
-
[8]
Sianos et
G. Sianos et. al: The SYNTAX Score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention1(2), 219–227 (2005)
2005
-
[9]
Gao, Y., Kim, S., McIntosh, C.: EchoingECG: An Electrocardiogram Cross-Modal Model for Echocardiogram Tasks, p. 175–185. Springer Nature Switzerland (Sep 2025).https://doi.org/10.1007/978-3-032-04971-1_17
-
[10]
Zhang, D
H. Zhang, D. Zhang, Z. Gao, and H. Zhang: Joint Segmentation and Quantification of Main Coronary Vessels Using Dual-Branch Multi-scale Attention Network. pp. 369–378. Springer-Verlag, Strasbourg, France (2021).https://doi.org/10.1007/ 978-3-030-87193-2_35 10 Nikola Cenikj et al
2021
-
[11]
Biomolecules14, 590 (05 2024).https: //doi.org/10.3390/biom14050590
Hua, L., Luo, Y., Qi, Q., Long, J.: Medicalclip: Anomaly-detection domain gen- eralization with asymmetric constraints. Biomolecules14, 590 (05 2024).https: //doi.org/10.3390/biom14050590
-
[12]
I. K. Lee, J. Shin, Y. Lee, J. Ku, and H. Kim: SSASS: Semi-Supervised Approach for Stenosis Segmentation (2023).https://doi.org/10.48550/arXiv.2311.10281
-
[13]
Li, J., Aguirre, A., Moura, J., Liu, C., Zhong, L., Sun, C., Clifford, G., Westover, B., Hong, S.: An electrocardiogram foundation model built on over 10 million recordings with external evaluation across multiple domains (2025).https://doi. org/10.48550/arXiv.2410.04133
-
[14]
https://doi.org/10.48550/arXiv.2509.10151
Lunelli, R., Nicolson, A., Pröll, S.M., Reinstadler, S.J., Bauer, A., Dlaska, C.: Benchecg and xecg: a benchmark and baseline for ecg foundation models (2025). https://doi.org/10.48550/arXiv.2509.10151
-
[15]
Learning Transferable Visual Models From Natural Language Supervision
Radford, A., Kim, J.W., Hallacy, C., Ramesh, A., Goh, G., Agarwal, S., Sastry, G., Askell, A., Mishkin, P., Clark, J., Krueger, G., Sutskever, I.: Learning transferable visual models from natural language supervision (2021).https://doi.org/10. 48550/arXiv.2103.00020
work page internal anchor Pith review Pith/arXiv arXiv 2021
-
[16]
https://doi.org/10.48550/arXiv.2506.20683
Selivanov, A., Müller, P., Özgün Turgut, Stolt-Ansó, N., Rückert, D.: Global and local contrastive learning for joint representations from cardiac mri and ecg (2025). https://doi.org/10.48550/arXiv.2506.20683
-
[17]
T. Han et. al: Coronary artery stenosis detection via proposal-shifted spatial- temporal transformer in X-ray angiography. Computers in Biology and Medicine 153, 106546 (2023).https://doi.org/10.1016/j.compbiomed.2023.106546
-
[18]
Özgün Turgut, Müller, P., Hager, P., Shit, S., Starck, S., Menten, M.J., Martens, E., Rueckert, D.: Unlocking the diagnostic potential of electrocardiograms through information transfer from cardiac magnetic resonance imaging (2025).https:// doi.org/10.48550/arXiv.2308.05764
-
[19]
Özgün Turgut, Müller, P., Menten, M.J., Rueckert, D.: Towards generalisable time series understanding across domains (2025).https://doi.org/10.48550/arXiv. 2410.07299
work page internal anchor Pith review doi:10.48550/arxiv 2025
-
[20]
V. V. Danilov et. al: Real-time coronary artery stenosis detection based on mod- ern neural networks. Scientific Reports11(1), 7582 (2021).https://doi.org/10. 1038/s41598-021-87174-2
2021
-
[21]
BMC Medical Informatics and Decision Making24(11 2024)
Xue, Z., Geng, S., Guo, S., Mu, G., Yu, B., Wang, P., Hu, S., Zhang, D., Xu, W., Liu, Y., Yang, L., Tao, H., Hong, S., Chen, K.: Screening for severe coro- nary stenosis in patients with apparently normal electrocardiograms based on deep learning. BMC Medical Informatics and Decision Making24(11 2024). https://doi.org/10.1186/s12911-024-02764-0
-
[22]
Computa- tional and Structural Biotechnology Journal27, 278–286 (2025).https://doi
Yeh, C.H., Tsai, T.H., Chen, C.H., Chou, Y.J., Mao, C.T., Su, T.P., Yang, N.I., Lai, C.C., Chen, C.T., Sytwu, H.K., Tsai, T.F.: Artificial intelligence-enhanced electrocardiography improves the detection of coronary artery disease. Computa- tional and Structural Biotechnology Journal27, 278–286 (2025).https://doi. org/10.1016/j.csbj.2024.12.032
-
[23]
Zhang, S., Xu, Y., Usuyama, N., Xu, H., Bagga, J., Tinn, R., Preston, S., Rao, R., Wei, M., Valluri, N., Wong, C., Tupini, A., Wang, Y., Mazzola, M., Shukla, S., Liden, L., Gao, J., Crabtree, A., Piening, B., Bifulco, C., Lungren, M.P., Naumann, T., Wang, S., Poon, H.: Biomedclip: a multimodal biomedical foundation model pretrained from fifteen million sc...
work page internal anchor Pith review Pith/arXiv arXiv doi:10.48550/arxiv.2303.00915 2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.