Point Cloud Segmentation for Autonomous Clip Positioning in Laparoscopic Cholecystectomy on a Phantom
Pith reviewed 2026-06-27 09:25 UTC · model grok-4.3
The pith
A point-cloud segmentation model trained on 60 real examples plus synthetic pre-training enables the first autonomous robotic clip positioning on a laparoscopic surgery phantom at 0.75 mm precision.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
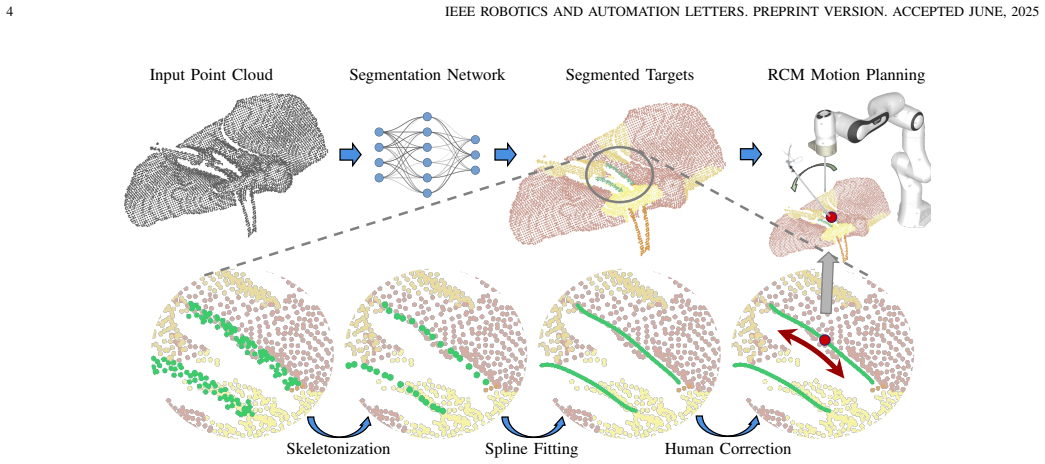
The central claim is that a segmentation model trained on only 60 hand-labeled real point clouds, after pre-training on 128,000 synthetic point clouds and two new augmentation methods, produces segmentations accurate enough to extract clip targets via spline interpolation and to drive a robot to those targets with 0.75 mm precision at 95 percent success while executing the full autonomous clip-positioning task at 100 percent success on a physical phantom.
What carries the argument
Colorless point-cloud segmentation model that identifies anatomical structures so spline interpolation can compute clip target positions from a single-camera view.
If this is right
- Target positions are localized to 0.75 mm at 95 percent success rate in robot experiments.
- Autonomous clip positioning completes with 100 percent success on the phantom.
- End-effector motion remains within minimally-invasive surgery constraints and is shown to the operator for verification.
- The same pipeline supplies insights for other surgical or non-surgical tasks that require precise target identification and navigation.
Where Pith is reading between the lines
- If the synthetic-plus-real training recipe generalizes, similar systems could be built for other clip or staple placement tasks without collecting hundreds of labeled surgical point clouds.
- The interpretability requirement (visualized motion paths) may become a standard filter for any autonomous surgical robot that must remain under human oversight.
- Extending the method to stereo or RGB-D input could reduce reliance on perfect point-cloud quality while preserving the low-data training strategy.
Load-bearing premise
The segmentation accuracy achieved on the phantom will remain high enough for safe clip placement when the same model is later used on real human tissue that differs in lighting, blood, and deformation.
What would settle it
A drop in segmentation accuracy below the level needed for 0.75 mm target localization when the trained model is tested on real-patient point clouds recorded under variable lighting and tissue deformation.
Figures



read the original abstract
High-risk applications in robotics, such as robot-assisted surgery, present unique challenges. These systems must be both highly precise and interpretable in order to be deployed in environments with very low tolerance for error or unsafe exploration. We present the first robotic system to demonstrate autonomous clip positioning on a physical phantom in laparoscopic surgery, one of the most common interventions in general surgery. After segmentation of a colorless point cloud from a single camera, target positions for the clips are extracted using spline interpolation, and can then be adjusted by the human operator. The segmentation model is trained on only 60 hand-labeled real point clouds, reflecting data scarcity in the surgical domain. We overcome this with a combination of pre-training on 128,000 synthetic point clouds and two novel data augmentation techniques. The motion of the end-effector to each target is visualized for the operator, satisfying the unique motion constraints of minimally-invasive surgery while ensuring that the robot's actions are verifiable and interpretable. In real robot experiments, our system localizes targets with the required precision of 0.75mm at a 95% success rate and executes autonomous clip positioning with a 100% success rate. We provide insights that are applicable to many other surgical and non-surgical tasks that require identifying and navigating to a precise target. Source code and project page: https://github.com/balazsgyenes/kirurc
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper presents the first robotic system for autonomous clip positioning on a physical phantom for laparoscopic cholecystectomy. It performs segmentation on colorless point clouds from a single camera using a model pre-trained on 128,000 synthetic clouds and fine-tuned on 60 hand-labeled real ones with two novel augmentations; targets are then extracted via spline interpolation (with optional human adjustment), and the end-effector motion is visualized for interpretability. Physical robot experiments on the phantom report 95% success localizing targets to the required 0.75 mm precision and 100% success executing autonomous clip positioning.
Significance. If the reported success rates hold under the described experimental conditions, the work supplies a concrete, reproducible demonstration of precise autonomous action in a data-scarce surgical robotics setting on a phantom, together with an interpretable visualization step that respects MIS constraints. The public release of source code and project page is a clear strength that supports verification and extension.
major comments (2)
- [Experiments / Results] Experiments / Results section: the manuscript states a 95% success rate at the 0.75 mm threshold and a 100% clip-positioning success rate but provides neither the number of trials performed, error bars or confidence intervals, nor an explicit definition of what constitutes a failure or how the 0.75 mm threshold was selected; these omissions are load-bearing for the central empirical claim.
- [Methods] Methods section on data augmentation: the two novel augmentation techniques are described only at a high level; without their precise algorithmic definitions or pseudocode (even though code is released), it is difficult to assess how they address the domain gap between synthetic and real point clouds that underpins the reported segmentation accuracy.
minor comments (1)
- [Abstract / Discussion] The abstract and title correctly limit all quantitative claims to the phantom; the discussion of applicability to real tissue should be framed explicitly as future work rather than as a basis for the reported results.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback. We address each major comment below and will revise the manuscript to strengthen the reporting of experiments and the description of the augmentation methods.
read point-by-point responses
-
Referee: [Experiments / Results] Experiments / Results section: the manuscript states a 95% success rate at the 0.75 mm threshold and a 100% clip-positioning success rate but provides neither the number of trials performed, error bars or confidence intervals, nor an explicit definition of what constitutes a failure or how the 0.75 mm threshold was selected; these omissions are load-bearing for the central empirical claim.
Authors: We agree that these statistical details are necessary to substantiate the central claims. In the revised manuscript we will explicitly state the number of trials performed for both localization and clip placement, report error bars or binomial confidence intervals, provide a clear definition of failure (localization error > 0.75 mm or any clip placement that does not meet the target), and justify the 0.75 mm threshold by reference to the clinical tolerance required for safe clip application on the cystic duct in laparoscopic cholecystectomy. revision: yes
-
Referee: [Methods] Methods section on data augmentation: the two novel augmentation techniques are described only at a high level; without their precise algorithmic definitions or pseudocode (even though code is released), it is difficult to assess how they address the domain gap between synthetic and real point clouds that underpins the reported segmentation accuracy.
Authors: We accept that a high-level description is insufficient for reproducibility and evaluation. The revised Methods section will include the precise algorithmic definitions of both augmentation techniques together with pseudocode, explicitly showing the operations applied to synthetic point clouds to reduce the domain gap before fine-tuning on the 60 real samples. revision: yes
Circularity Check
No significant circularity
full rationale
The paper reports empirical success rates (95% localization at 0.75 mm, 100% clip positioning) measured directly in physical robot experiments on a phantom. The segmentation model is trained on 60 real + 128k synthetic point clouds with data augmentation, but the central claims are experimental outcomes on the physical setup rather than any derivation, equation, or prediction that reduces to its own fitted inputs by construction. No self-citations, uniqueness theorems, or ansatzes are invoked to support the reported performance; the results stand as direct measurements independent of any circular reduction.
Axiom & Free-Parameter Ledger
free parameters (1)
- number of real labeled point clouds
axioms (1)
- domain assumption A single colorless point cloud from one camera is sufficient to identify clip target locations on the phantom anatomy.
Reference graph
Works this paper leans on
-
[1]
Epidemiology of gallbladder stone disease,
E. A. Shaffer, “Epidemiology of gallbladder stone disease,”Best Practice & Research Clinical Gastroenterology, pp. 981–996, Jan. 2006
2006
-
[2]
Autonomy for Surgical Robots: Concepts and Paradigms,
T. Haidegger, “Autonomy for Surgical Robots: Concepts and Paradigms,” IEEE Transactions on Medical Robotics and Bionics, 2019
2019
-
[3]
Point cloud models improve visual robustness in robotic learners,
S. Peri, I. Lee, C. Kim, L. Fuxin, T. Hermans, and S. Lee, “Point cloud models improve visual robustness in robotic learners,”ICRA, 2024
2024
-
[4]
DexPoint: General- izable Point Cloud Reinforcement Learning for Sim-to-Real Dexterous Manipulation,
Y . Qin, B. Huang, Z.-H. Yin, H. Su, and X. Wang, “DexPoint: General- izable Point Cloud Reinforcement Learning for Sim-to-Real Dexterous Manipulation,” inCoRL, Mar. 2023
2023
-
[5]
Real-time deep learning semantic segmentation during intra-operative surgery for 3D augmented reality assistance,
L. Tanzi, P. Piazzolla, F. Porpiglia, and E. Vezzetti, “Real-time deep learning semantic segmentation during intra-operative surgery for 3D augmented reality assistance,”IJCARS, Sept. 2021
2021
-
[6]
Autonomous Tissue Retraction in Robotic Assisted Minimally Invasive Surgery – A Feasibility Study,
A. Attanasio, B. Scaglioni, M. Leonetti, A. F. Frangi, W. Cross, C. S. Biyani, and P. Valdastri, “Autonomous Tissue Retraction in Robotic Assisted Minimally Invasive Surgery – A Feasibility Study,”RAL, Oct. 2020
2020
-
[7]
A Comparative Study of Spatio-Temporal U-Nets for Tissue Segmentation in Surgical Robotics,
A. Attanasio, C. Alberti, B. Scaglioni, N. Marahrens, A. F. Frangi, M. Leonetti, C. S. Biyani, E. De Momi, and P. Valdastri, “A Comparative Study of Spatio-Temporal U-Nets for Tissue Segmentation in Surgical Robotics,”IEEE Trans. on Medical Robotics and Bionics, Feb. 2021
2021
-
[8]
An Automatic Path Planning Method of Pedicle Screw Placement Based on Preoperative CT Images,
X. Qi, J. Meng, M. Li, Y . Yang, Y . Hu, B. Li, J. Zhang, and W. Tian, “An Automatic Path Planning Method of Pedicle Screw Placement Based on Preoperative CT Images,”IEEE Trans. on Medical Robotics and Bionics, May 2022
2022
-
[9]
Autonomous Needle Manipulation for Robotic Surgical Suturing Based on Skills Learned from Demonstration,
K. L. Schwaner, D. Dall’Alba, P. T. Jensen, P. Fiorini, and T. R. Savarimuthu, “Autonomous Needle Manipulation for Robotic Surgical Suturing Based on Skills Learned from Demonstration,” inCASE, Aug. 2021
2021
-
[10]
A Learning-Driven Framework with Spatial Optimization For Surgical Suture Thread Reconstruction and Autonomous Grasping Under Multiple Topologies and Environmental Noises,
B. Lu, W. Chen, Y .-M. Jin, D. Zhang, Q. Dou, H. K. Chu, P.-A. Heng, and Y .-H. Liu, “A Learning-Driven Framework with Spatial Optimization For Surgical Suture Thread Reconstruction and Autonomous Grasping Under Multiple Topologies and Environmental Noises,” inIROS, Oct. 2020
2020
-
[11]
Estimating Reference Bony Shape Models for Orthognathic Surgical Planning Using 3D Point-Cloud Deep Learning,
D. Xiao, C. Lian, H. Deng, T. Kuang, Q. Liu, L. Ma, D. Kim, Y . Lang, X. Chen, J. Gateno, S. G. Shen, J. J. Xia, and P.-T. Yap, “Estimating Reference Bony Shape Models for Orthognathic Surgical Planning Using 3D Point-Cloud Deep Learning,”IEEE Journal of Biomedical and Health Informatics, vol. 25, no. 8, pp. 2958–2966, Aug. 2021
2021
-
[12]
6DOF Needle Pose Estimation for Robot-Assisted Vitreoretinal Surgery,
M. Zhou, X. Hao, A. Eslami, K. Huang, C. Cai, C. P. Lohmann, N. Navab, A. Knoll, and M. A. Nasseri, “6DOF Needle Pose Estimation for Robot-Assisted Vitreoretinal Surgery,”IEEE Access, 2019
2019
-
[13]
SuPer: A Surgical Perception Framework for Endoscopic Tissue Manipulation With Surgical Robotics,
Y . Li, F. Richter, J. Lu, E. K. Funk, R. K. Orosco, J. Zhu, and M. C. Yip, “SuPer: A Surgical Perception Framework for Endoscopic Tissue Manipulation With Surgical Robotics,”RAL, vol. 5, Apr. 2020
2020
-
[14]
Learning Visual Shape Control of Novel 3D Deformable Objects from Partial-View Point Clouds,
B. Thach, B. Y . Cho, A. Kuntz, and T. Hermans, “Learning Visual Shape Control of Novel 3D Deformable Objects from Partial-View Point Clouds,” inICRA, May 2022
2022
-
[15]
Autonomous robotic laparoscopic surgery for intestinal anastomosis,
H. Saeidi, J. D. Opfermann, M. Kam, S. Wei, S. Leonard, M. H. Hsieh, J. U. Kang, and A. Krieger, “Autonomous robotic laparoscopic surgery for intestinal anastomosis,”Science Robotics, p. eabj2908, Jan. 2022
2022
-
[16]
PointNet: Deep Learning on Point Sets for 3D Classification and Segmentation,
C. R. Qi, H. Su, K. Mo, and L. J. Guibas, “PointNet: Deep Learning on Point Sets for 3D Classification and Segmentation,” inCVPR, 2017
2017
-
[17]
Point Trans- former,
H. Zhao, L. Jiang, J. Jia, P. H. S. Torr, and V . Koltun, “Point Trans- former,” inCVPR, 2021
2021
-
[18]
Dynamic Graph CNN for Learning on Point Clouds,
Y . Wang, Y . Sun, Z. Liu, S. E. Sarma, M. M. Bronstein, and J. M. Solomon, “Dynamic Graph CNN for Learning on Point Clouds,”ACM Trans. Graph., vol. 38, no. 5, pp. 146:1–146:12, Oct. 2019
2019
-
[19]
Masked Autoencoders for Point Cloud Self-supervised Learning,
Y . Pang, W. Wang, F. E. H. Tay, W. Liu, Y . Tian, and L. Yuan, “Masked Autoencoders for Point Cloud Self-supervised Learning,” inECCV, 2022
2022
-
[20]
Point-BERT: Pre- Training 3D Point Cloud Transformers With Masked Point Modeling,
X. Yu, L. Tang, Y . Rao, T. Huang, J. Zhou, and J. Lu, “Point-BERT: Pre- Training 3D Point Cloud Transformers With Masked Point Modeling,” inCVPR, 2022
2022
-
[21]
Improved Regularization of Convolutional Neural Networks with Cutout
T. DeVries and G. W. Taylor, “Improved regularization of convolutional neural networks with cutout,”arXiv preprint arXiv:1708.04552, 2017
work page internal anchor Pith review Pith/arXiv arXiv 2017
-
[22]
LapGym - An Open Source Framework for Re- inforcement Learning in Robot-Assisted Laparoscopic Surgery,
P. M. Scheikl, B. Gyenes, R. Younis, C. Haas, G. Neumann, M. Wagner, and F. Mathis-Ullrich, “LapGym - An Open Source Framework for Re- inforcement Learning in Robot-Assisted Laparoscopic Surgery,”JMLR, 2023
2023
-
[23]
Point Cloud Skeletons via Laplacian Based Contraction,
J. Cao, A. Tagliasacchi, M. Olson, H. Zhang, and Z. Su, “Point Cloud Skeletons via Laplacian Based Contraction,” in2010 Shape Modeling International Conference, June 2010, pp. 187–197
2010
-
[24]
Point Cloud Augmentation With Weighted Local Transformations,
S. Kim, S. Lee, D. Hwang, J. Lee, S. J. Hwang, and H. J. Kim, “Point Cloud Augmentation With Weighted Local Transformations,” inICCV, 2021
2021
-
[25]
PointNet++: Deep Hierarchical Feature Learning on Point Sets in a Metric Space,
C. R. Qi, L. Yi, H. Su, and L. J. Guibas, “PointNet++: Deep Hierarchical Feature Learning on Point Sets in a Metric Space,” inNeurIPS. Curran Associates, Inc., 2017
2017
-
[26]
Stratified transformer for 3d point cloud segmentation,
X. Lai, J. Liu, L. Jiang, L. Wang, H. Zhao, S. Liu, X. Qi, and J. Jia, “Stratified transformer for 3d point cloud segmentation,” inCVPR, 2022
2022
-
[27]
Stereo reconstruction from microscopic images for computer-assisted ophthalmic surgery,
R. Peter, S. Moreira, E. Tagliabue, M. Hillenbrand, R. G. Nunes, and F. Mathis-Ullrich, “Stereo reconstruction from microscopic images for computer-assisted ophthalmic surgery,”IJCARS, Mar. 2025
2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.