Transformer-Guided Graph Attention for Direct Cardiac Mesh Reconstruction: A Structural Digital Twin Framework
Pith reviewed 2026-06-27 07:12 UTC · model grok-4.3
The pith
An end-to-end network produces simulation-ready cardiac surface meshes directly from 3D CT or MRI by deforming a fixed template with a graph attention head.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
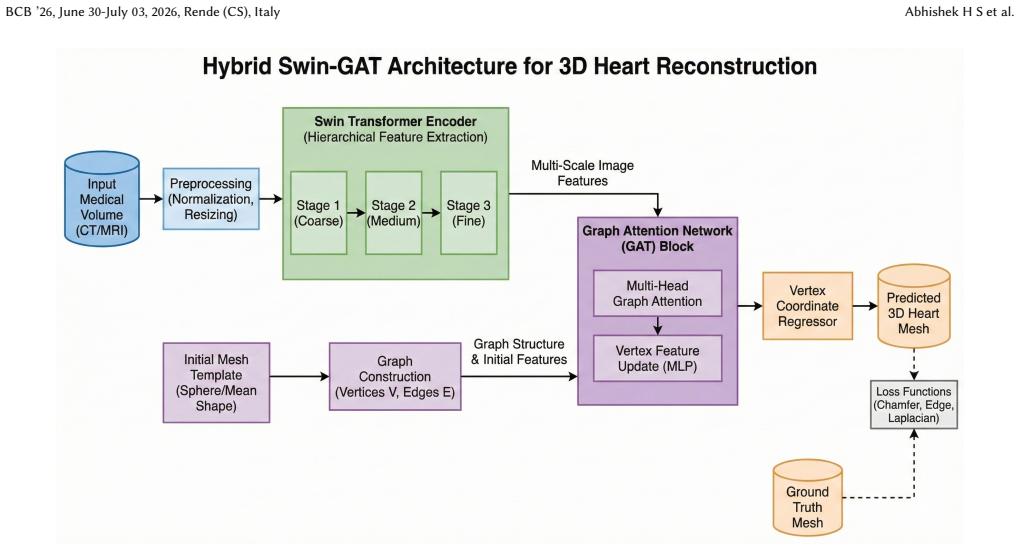
The authors present a 3D Swin Transformer encoder-decoder that extracts volumetric features from CT or MRI, which then drive a Graph Attention Network head to iteratively deform a template mesh until it matches the patient's cardiac boundaries, producing smooth, simulation-ready surfaces in a single forward pass.
What carries the argument
The Graph Attention Network head that iteratively deforms a fixed template mesh using features supplied by the 3D Swin Transformer encoder-decoder.
If this is right
- Every mesh exits the network ready for immediate use in cardiac simulations without additional smoothing or repair.
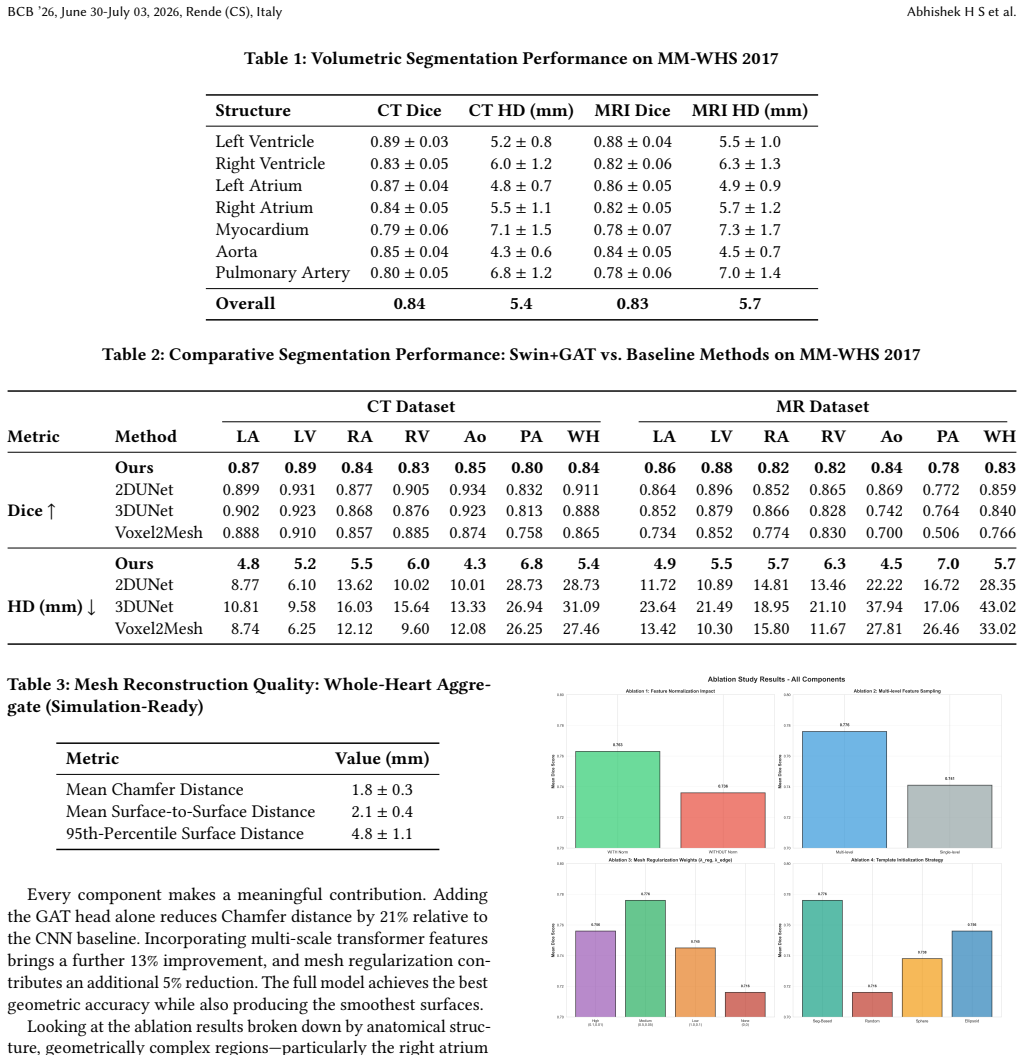
- The same trained model handles both CT and MRI inputs while maintaining competitive Dice scores of 0.84 and 0.83 respectively.
- Mesh quality metrics (Chamfer distance 1.8 mm) become the primary evaluation target rather than pixel-wise segmentation accuracy.
- The workflow removes operator-dependent post-processing, reducing the specialist time required to build patient-specific models.
Where Pith is reading between the lines
- The template-deformation strategy could be tested on other tubular or surface-based anatomies where a canonical starting mesh exists.
- Real-time clinical deployment would require measuring inference latency on standard hospital hardware to confirm the single-pass advantage.
- Direct comparison of simulation outputs from these meshes versus traditionally cleaned meshes would quantify any downstream accuracy gain or loss.
Load-bearing premise
A single fixed template mesh can be deformed by attention updates to match the cardiac anatomy of every patient while remaining topologically correct and free of self-intersections.
What would settle it
Generating meshes on a held-out set of diverse cardiac scans and finding a substantial fraction with non-manifold surfaces, holes, or 95th-percentile surface distances well above 5 mm would falsify the claim of reliable direct reconstruction.
Figures



read the original abstract
Building patient-specific cardiac models sits at the heart of precision cardiology, yet getting those models into clinical use keeps running into the same wall: mesh generation is slow, messy, and frustrating. The standard workflow -- segmenting the image, running Marching Cubes, and then manually cleaning up the result -- is time-consuming, inconsistent across operators, and demands specialist knowledge most clinical teams do not have. We take a fundamentally different approach. Instead of treating segmentation and mesh generation as two separate problems, we train a single end-to-end network that goes directly from a raw 3D medical image to a smooth, simulation-ready cardiac surface mesh. The core is a 3D Swin Transformer encoder-decoder that extracts volumetric features from CT or MRI volumes, paired with a Graph Attention Network (GAT) head that iteratively deforms a template mesh to fit the patient's cardiac boundary. We tested on the MM-WHS 2017 benchmark using both CT and MRI. Segmentation scores were competitive (Dice of 0.84 on CT, 0.83 on MRI), but the primary focus is mesh quality: mean Chamfer distance of 1.8 mm, with 95th-percentile surface distance below 5 mm. Every mesh is produced in a single forward pass -- no Marching Cubes, no smoothing filters, no manual cleanup. We argue that for cardiac digital twin pipelines, geometric fidelity and topological correctness matter more than pixel-level Dice scores. By removing the post-processing bottleneck, this approach makes patient-specific cardiac simulation substantially more accessible for clinical use.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes an end-to-end network for direct reconstruction of cardiac surface meshes from raw 3D CT/MRI volumes. It combines a 3D Swin Transformer encoder-decoder for volumetric feature extraction with a Graph Attention Network (GAT) head that iteratively deforms a fixed template mesh to match patient anatomy. On the MM-WHS 2017 benchmark the method reports Dice scores of 0.84 (CT) and 0.83 (MRI) together with mesh quality metrics of 1.8 mm mean Chamfer distance and 95th-percentile surface distance below 5 mm, claiming that every output is simulation-ready without Marching Cubes, smoothing, or manual cleanup.
Significance. If the experimental claims are substantiated, the work would address a practical bottleneck in cardiac digital-twin pipelines by removing the post-processing stage between image and usable surface mesh. The transformer-plus-GAT architecture is a plausible route to topology-preserving deformation, and the reported aggregate distances are competitive with existing pipelines. However, the absence of any topology audit, split information, or baseline comparison in the provided description prevents a firm judgment on whether the central claim is supported.
major comments (2)
- [Abstract] Abstract: the claim that the GAT head produces topologically correct, manifold meshes for every patient rests on the unverified assumption that a single fixed template can be deformed without self-intersections or non-manifold edges across all anatomical variations in MM-WHS 2017; no per-case topology audit, invalid-mesh count, or regularization term enforcing manifoldness is mentioned.
- [Abstract] Abstract: the reported Chamfer and surface-distance figures are presented without any description of training/validation splits, baseline methods, ablation studies, or error analysis, so it is impossible to determine whether the metrics actually support the assertion of reliable direct mesh reconstruction.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback on the abstract claims. We address each major comment below and will revise the manuscript to strengthen the presentation of topology verification and experimental details.
read point-by-point responses
-
Referee: [Abstract] Abstract: the claim that the GAT head produces topologically correct, manifold meshes for every patient rests on the unverified assumption that a single fixed template can be deformed without self-intersections or non-manifold edges across all anatomical variations in MM-WHS 2017; no per-case topology audit, invalid-mesh count, or regularization term enforcing manifoldness is mentioned.
Authors: We agree that the current manuscript does not report a per-case topology audit or any regularization term for manifoldness. In the revised version we will add a dedicated analysis on the MM-WHS 2017 test set that counts self-intersections and non-manifold edges for every output mesh. If any invalid meshes are found we will introduce an appropriate regularization term into the training loss. This will directly substantiate the simulation-ready claim. revision: yes
-
Referee: [Abstract] Abstract: the reported Chamfer and surface-distance figures are presented without any description of training/validation splits, baseline methods, ablation studies, or error analysis, so it is impossible to determine whether the metrics actually support the assertion of reliable direct mesh reconstruction.
Authors: The abstract is intentionally concise. The full manuscript already details the official MM-WHS 2017 train/test split, quantitative comparisons against voxel-to-mesh baselines, ablation studies isolating the Swin Transformer and GAT components, and per-case error breakdowns. We will revise the abstract to include a one-sentence reference to the evaluation protocol and point readers to the Experiments section for the complete splits, baselines, ablations, and error analysis. revision: yes
Circularity Check
No circularity: standard supervised DL pipeline with no derivations or self-referential steps
full rationale
The paper presents an end-to-end neural network (3D Swin Transformer encoder-decoder + GAT head for template mesh deformation) trained supervised on MM-WHS 2017 data. No equations, derivations, fitted parameters renamed as predictions, or load-bearing self-citations appear in the provided text. Performance claims (Chamfer distance, Dice) are empirical evaluation results, not reductions by construction. The fixed-template deformation is an architectural assumption, not a mathematical step that collapses to its inputs. This matches the default expectation of a non-circular ML methods paper.
Axiom & Free-Parameter Ledger
free parameters (1)
- Template mesh initialization
axioms (1)
- domain assumption The MM-WHS 2017 dataset is representative of the variability encountered in clinical cardiac CT and MRI scans
Reference graph
Works this paper leans on
-
[1]
The ‘Digital Twin’ to Enable the Vision of Precision Cardiology,
J. Corral-Acero et al., “The ‘Digital Twin’ to Enable the Vision of Precision Cardiology, ”European Heart Journal, vol. 41, no. 48, pp. 4556–4564, 2020
2020
-
[2]
Building Digital Twins for Cardiovascular Health: From Principles to Clinical Impact,
K. Sel et al., “Building Digital Twins for Cardiovascular Health: From Principles to Clinical Impact, ”Journal of the American Heart Association, vol. 13, no. 19, e032981, 2024
2024
-
[3]
Deep Learning for Cardiac Image Segmentation: A Review,
C. Chen et al., “Deep Learning for Cardiac Image Segmentation: A Review, ” Frontiers in Cardiovascular Medicine, vol. 7, 2020
2020
-
[4]
Deep Neural Network Architectures for Cardiac Image Segmentation: A Review,
J. El-Taraboulsi et al., “Deep Neural Network Architectures for Cardiac Image Segmentation: A Review, ”Machine Learning with Applications, vol. 13, 100476, 2023
2023
-
[5]
A Review of Segmentation Methods in Short-Axis Cardiac MR Images,
C. Petitjean and J.-N. Dacher, “A Review of Segmentation Methods in Short-Axis Cardiac MR Images, ”Medical Image Analysis, vol. 15, no. 2, pp. 169–184, 2011
2011
-
[6]
A Review of Heart Chamber Segmentation for Structural and Func- tional Analysis Using Cardiac Magnetic Resonance Imaging,
P. Peng et al., “A Review of Heart Chamber Segmentation for Structural and Func- tional Analysis Using Cardiac Magnetic Resonance Imaging, ”Magnetic Resonance Materials in Physics, Biology and Medicine, vol. 29, no. 2, pp. 155–195, 2016. 8 Transformer-Guided Graph Attention for Direct Cardiac Mesh Reconstruction: A Structural Digital Twin Framework BCB ’2...
2016
-
[7]
Evaluation of Algorithms for Multi-Modality Whole Heart Segmentation: An Open-Access Grand Challenge,
X. Zhuang and J. Shen, “Evaluation of Algorithms for Multi-Modality Whole Heart Segmentation: An Open-Access Grand Challenge, ”Medical Image Analysis, vol. 58, 101537, 2019
2019
-
[8]
Marching Cubes: A High Resolution 3D Surface Construction Algorithm,
W. E. Lorensen and H. E. Cline, “Marching Cubes: A High Resolution 3D Surface Construction Algorithm, ” inProc. ACM SIGGRAPH, 1987, pp. 163–169
1987
-
[9]
U-Net: Convolutional Networks for Biomedical Image Segmentation,
O. Ronneberger, P. Fischer, and T. Brox, “U-Net: Convolutional Networks for Biomedical Image Segmentation, ” inProc. MICCAI, 2015, pp. 234–241
2015
-
[10]
3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation,
Ö. Çiçek et al., “3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation, ” inProc. MICCAI, 2016, pp. 424–432
2016
-
[11]
V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation,
F. Milletari, N. Navab, and S.-A. Ahmadi, “V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation, ” inProc. 3DV, 2016, pp. 565–571
2016
-
[12]
nnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation,
F. Isensee et al., “nnU-Net: A Self-Configuring Method for Deep Learning-Based Biomedical Image Segmentation, ”Nature Methods, vol. 18, pp. 203–211, 2021
2021
-
[13]
Swin Transformer: Hierarchical Vision Transformer Using Shifted Windows,
Z. Liu et al., “Swin Transformer: Hierarchical Vision Transformer Using Shifted Windows, ” inProc. ICCV, 2021, pp. 9992–10002
2021
-
[14]
Swin UNETR: Swin Transformers for Semantic Segmenta- tion of Brain Tumors in MRI Images,
A. Hatamizadeh et al., “Swin UNETR: Swin Transformers for Semantic Segmenta- tion of Brain Tumors in MRI Images, ” inProc. MICCAI BrainLes Workshop, LNCS, vol. 12962, pp. 272–284, 2022
2022
-
[15]
Three-Dimensional Printed Models for Surgical Planning of Complex Congenital Heart Defects,
I. Valverde et al., “Three-Dimensional Printed Models for Surgical Planning of Complex Congenital Heart Defects, ”European Journal of Cardio-Thoracic Surgery, vol. 52, no. 6, pp. 1139–1148, 2017
2017
-
[16]
3D-Manufactured Patient-Specific Models of Congenital Heart Defects,
G. Biglino et al., “3D-Manufactured Patient-Specific Models of Congenital Heart Defects, ”BMJ Open, vol. 5, e007165, 2015
2015
-
[17]
Three-Dimensional Printing in Congenital Heart Disease: A Systematic Review,
I. W. W. Lau et al., “Three-Dimensional Printing in Congenital Heart Disease: A Systematic Review, ”Journal of Magnetic Resonance Imaging, vol. 49, no. 4, pp. 1005–1019, 2019
2019
-
[18]
Three-Dimensional Printing for Cardiovascular Diseases,
H. Wang et al., “Three-Dimensional Printing for Cardiovascular Diseases, ” Biomedical Engineering Online, vol. 19, 2020
2020
-
[19]
Graph Attention Networks,
P. Veličković et al., “Graph Attention Networks, ” inProc. ICLR, 2018
2018
-
[20]
MeshCNN: A Network with an Edge,
R. Hanocka et al., “MeshCNN: A Network with an Edge, ”ACM Transactions on Graphics (SIGGRAPH), vol. 38, no. 4, 2019
2019
-
[21]
Dense Graph Convolutional Networks on 3D Meshes,
W. Tang et al., “Dense Graph Convolutional Networks on 3D Meshes, ”Image and Vision Computing, vol. 112, 104190, 2021
2021
-
[22]
Multi-Modality Whole Heart Segmentation (MM-WHS 2017) Dataset,
X. Zhuang et al., “Multi-Modality Whole Heart Segmentation (MM-WHS 2017) Dataset, ” MICCAI Challenge, 2017
2017
-
[23]
Voxel2Mesh: 3D Mesh Model Generation from Single Images,
U. Wickramasinghe, F. Remelli, P. Knott, and P. Fua, “Voxel2Mesh: 3D Mesh Model Generation from Single Images, ” inProc. Medical Image Computing and Computer-Assisted Intervention (MICCAI), pp. 299–308, 2020
2020
-
[24]
Do LLMs Surpass Encoders for Biomedical NER?Proceedings
A. Balasubramanyam, R. Manwani, D. Kalyanpur, P. B. Basavaraju, S. V. Padmaraju, and P. B. Honnavalli, “A Cardiovascular Modeling Framework for Enabling Personalized Healthcare: A Digital Twin Approach, ” inProc. IEEE 13th Int. Conf. Healthcare Informatics (ICHI), 2025, pp. 478–489, doi: 10.1109/ICHI64645.2025.00062. 9
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.