DXA-Derived Skeletal Phenotypes and Hip Fracture Risk: A Backdoor-Adjusted Causal Analysis
Pith reviewed 2026-06-28 19:45 UTC · model grok-4.3
The pith
Total femur BMC and BMD show the largest backdoor-adjusted effects on hip fracture risk among 16 DXA phenotypes.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
Among the sixteen phenotypes, total femur BMC and total femur BMD exhibited the largest backdoor-adjusted ATEs of -0.0047 risk difference per SD increase. Clinical variables plus the top 11 ATE-ranked phenotypes achieved an AUC of 0.842 versus 0.709 for FRAX with femoral neck BMD, with higher sensitivity and similar specificity.
What carries the argument
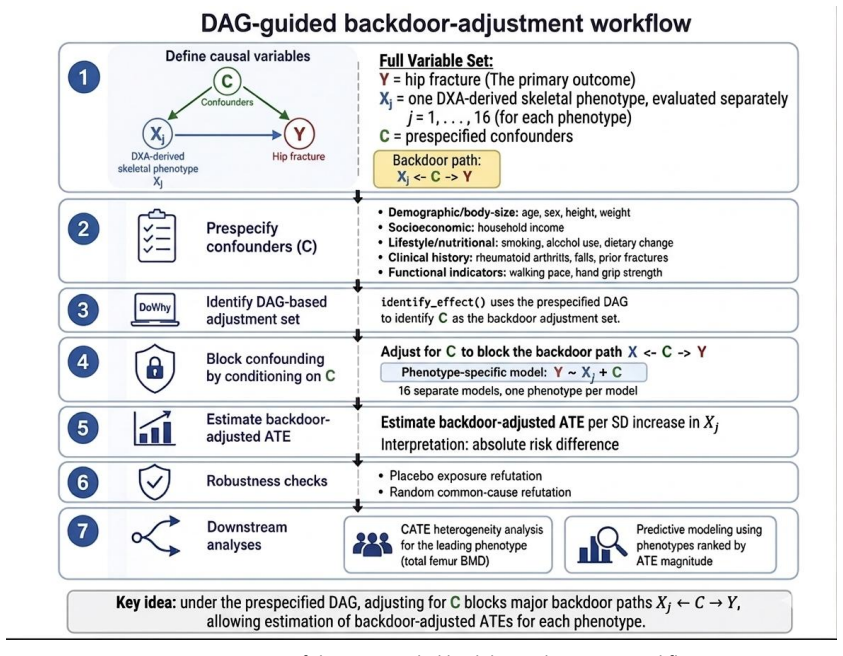
Backdoor-adjusted average treatment effect on the absolute risk-difference scale, obtained by fitting models that block all paths from each phenotype to hip fracture according to a prespecified DAG.
If this is right
- Total femur BMC and total femur BMD are the two phenotypes with the strongest protective associations on the risk-difference scale.
- Prediction models that combine clinical variables with the eleven highest-ATE phenotypes outperform FRAX with femoral neck BMD.
- The protective association of total femur BMD is larger among older participants and those with lower BMI.
- DXA hip phenotypes are not interchangeable for risk stratification once confounder adjustment is applied.
Where Pith is reading between the lines
- Existing DXA scans could be re-processed to report total femur BMC and BMD routinely if the ranking holds in other cohorts.
- If the DAG omits important selection effects from the linked health records, the reported ATEs could be biased.
- Testing whether the same phenotype ranking appears when the outcome is changed to vertebral or wrist fracture would check whether the findings are hip-specific.
Load-bearing premise
The prespecified DAG captures every confounder that affects both the DXA phenotypes and hip fracture risk, so that the backdoor criterion holds and no unmeasured confounding remains.
What would settle it
An observational study or trial that measures an additional variable strongly linked to both a top-ranked phenotype and to hip fracture incidence, then shows that including it materially changes the ATE estimates.
Figures
read the original abstract
Purpose: To compare dual-energy X-ray absorptiometry (DXA)-derived hip skeletal phenotypes in relation to hip fracture risk using prespecified confounder adjustment and to assess whether phenotypes ranked by their backdoor-adjusted average treatment effects (ATEs) improve risk stratification. Methods: We analyzed 21,098 UK Biobank participants with linked health records, hip DXA-derived skeletal measures, and prespecified covariates. Sixteen phenotypes spanning bone mineral content (BMC), bone mineral density (BMD), and T-score across hip-related regions were evaluated. Confounder selection was guided by a prespecified directed acyclic graph (DAG). Backdoor-adjusted ATEs were estimated on the absolute risk-difference scale per standard deviation (SD) increase. Effect heterogeneity was evaluated for total femur BMD, and downstream prediction was assessed using clinical variables combined with phenotypes ranked by ATE magnitude. Results: Among 21,098 participants, 115 had hip fractures. All 16 phenotypes showed negative backdoor-adjusted ATEs per SD increase. The largest ATEs were observed for total femur BMC and total femur BMD, each with a risk difference of -0.0047, corresponding to approximately 4.7 fewer hip fractures per 1,000 participants per SD higher phenotype value. Conditional effects of total femur BMD were stronger among older participants and those with lower BMI. In prediction, clinical variables plus the top 11 ATE-ranked phenotypes achieved higher AUC than FRAX with femoral neck BMD (0.842 vs. 0.709), with higher sensitivity (0.748 vs. 0.443) and similar specificity (0.793 vs. 0.777). Conclusion: DXA-derived hip skeletal phenotypes differed in their backdoor-adjusted ATEs. Phenotype-level causal evaluation may help identify informative DXA measures for risk stratification.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript claims that among 16 DXA-derived hip skeletal phenotypes analyzed in 21,098 UK Biobank participants (115 hip fractures), all show negative backdoor-adjusted ATEs on absolute hip fracture risk per SD increase, with total femur BMC and total femur BMD having the largest effects (-0.0047 risk difference each); adding the top 11 ATE-ranked phenotypes to clinical variables yields an AUC of 0.842 (vs. 0.709 for FRAX with femoral neck BMD), with improved sensitivity.
Significance. If the prespecified DAG is valid and the backdoor criterion holds with no unmeasured confounding or selection bias, the phenotype-specific ATE ranking and the reported AUC lift could provide a principled way to prioritize DXA measures for hip fracture risk stratification beyond standard clinical tools.
major comments (2)
- [Methods (confounder selection and DAG)] Methods section on confounder selection and DAG: The ATE point estimates (e.g., -0.0047 for total femur BMC/BMD) and their ranking rest entirely on the assumption that the prespecified DAG blocks all backdoor paths and satisfies the backdoor criterion with no residual unmeasured confounding; the manuscript provides no DAG validation, sensitivity analyses for unmeasured confounding, or robustness checks, which is load-bearing given only 115 events where even modest residual bias could reverse ordering or nullify effects.
- [Results (prediction)] Results (prediction and AUC section): The claim of AUC improvement to 0.842 (vs. 0.709) when adding the top 11 ATE-ranked phenotypes does not specify whether phenotype selection was performed within cross-validation folds, how the 115 events were handled in the absolute-risk models, or whether the gain survives adjustment for selection-induced optimism; this undermines the downstream risk-stratification conclusion.
minor comments (2)
- [Abstract] Abstract: The statement that 'all 16 phenotypes showed negative backdoor-adjusted ATEs' would benefit from reporting the range or at least one smaller-magnitude example to convey effect-size heterogeneity.
- [Methods] Notation: The risk-difference scale is clearly defined, but the manuscript should explicitly state whether the ATEs are marginal or conditional on the full covariate set used in the backdoor adjustment.
Simulated Author's Rebuttal
We thank the referee for the constructive comments. We address each major point below and will revise the manuscript accordingly to improve transparency and robustness.
read point-by-point responses
-
Referee: [Methods (confounder selection and DAG)] Methods section on confounder selection and DAG: The ATE point estimates (e.g., -0.0047 for total femur BMC/BMD) and their ranking rest entirely on the assumption that the prespecified DAG blocks all backdoor paths and satisfies the backdoor criterion with no residual unmeasured confounding; the manuscript provides no DAG validation, sensitivity analyses for unmeasured confounding, or robustness checks, which is load-bearing given only 115 events where even modest residual bias could reverse ordering or nullify effects.
Authors: We agree that the ATE estimates and ranking depend on the DAG assumptions and that the modest event count (115 fractures) warrants caution. The DAG was prespecified from literature on hip fracture risk factors and DXA phenotypes. In revision we will add the DAG as a supplementary figure, expand the methods to detail backdoor path blocking, and include E-value sensitivity analyses to assess robustness to unmeasured confounding. We will also strengthen the limitations section to discuss implications of the event count for effect ordering stability. These additions will be made in the revised manuscript. revision: yes
-
Referee: [Results (prediction)] Results (prediction and AUC section): The claim of AUC improvement to 0.842 (vs. 0.709) when adding the top 11 ATE-ranked phenotypes does not specify whether phenotype selection was performed within cross-validation folds, how the 115 events were handled in the absolute-risk models, or whether the gain survives adjustment for selection-induced optimism; this undermines the downstream risk-stratification conclusion.
Authors: The referee is correct that the current description omits key methodological details on cross-validation and optimism. Phenotype ranking was performed on the full sample, which risks selection-induced optimism. We will revise the prediction section to implement nested cross-validation with ATE-based phenotype selection performed inside each training fold only. We will clarify use of logistic models for absolute risk with the binary outcome (115 events), report bootstrap- or CV-based optimism-adjusted AUC, sensitivity, and specificity, and update the results and discussion accordingly. revision: yes
Circularity Check
No significant circularity; derivation uses prespecified DAG and standard backdoor adjustment without reduction to inputs by construction
full rationale
The paper estimates backdoor-adjusted ATEs via a prespecified DAG for confounder selection, then ranks phenotypes by those ATEs for a downstream prediction model whose AUC is compared to FRAX. This does not match any enumerated circularity pattern: the ATE computation follows the standard backdoor formula on the given DAG rather than defining the outcome in terms of itself; the prediction step incorporates ATE-ranked variables but does not reduce the reported AUC gain to a tautology or fitted input renamed as prediction, as the benchmark is an external score and the model adds clinical variables. No self-citation load-bearing, uniqueness imported from authors, ansatz smuggling, or renaming of known results appears in the text. The central result therefore remains self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption The prespecified DAG satisfies the backdoor criterion for all 16 phenotypes with respect to hip fracture.
- domain assumption No unmeasured confounding or selection bias remains after adjustment.
Reference graph
Works this paper leans on
-
[1]
Under this framework, all evaluated phenotypes showed negative backdoor -adjusted ATEs per SD increase, with total femur BMC and total femur BMD showing the largest inverse ATEs
Conclusion This study used a prespecified DAG -guided backdoor -adjustment framework to evaluate 16 DXA - derived hip skeletal phenotypes in relation to hip fracture risk in the UK Biobank. Under this framework, all evaluated phenotypes showed negative backdoor -adjusted ATEs per SD increase, with total femur BMC and total femur BMD showing the largest in...
-
[2]
Parker M, Johansen A. Hip fracture. Bmj. 2006;333(7557):27–30. doi: 10.1136/bmj.333.7557.27. PubMed PMID: 16809710; PubMed Central PMCID: PMC1488757
-
[3]
Shaik A, Larsen K, Lane NE, Zhao C, Su KJ, Keyak JH, Tian Q, Sha Q, Shen H, Deng HW, Zhou W. A staged approach using machine learning and uncertainty quantification to predict the risk of hip fracture. Bone Rep. 2024;22:101805. Epub 20240912. doi: 10.1016/j.bonr.2024.101805. PubMed PMID: 39328352; PubMed Central PMCID: PMC11426051
-
[4]
Sing CW, Lin TC, Bartholomew S, Bell JS, Bennett C, Beyene K, Bosco -Levy P, Bradbury BD, Chan AHY, Chandran M, Cooper C, de Ridder M, Doyon CY, Droz-Perroteau C, Ganesan G, Hartikainen S, Ilomaki J, Jeong HE, Kiel DP, Kubota K, Lai EC, Lange JL, Lewiecki EM, Lin J, Liu J, Maskell J, de Abreu MM, O'Kelly J, Ooba N, Pedersen AB, Prats-Uribe A, Prieto-Alham...
-
[5]
Papadimitriou N, Tsilidis KK, Orfanos P, Benetou V, Ntzani EE, Soerjomataram I, Künn -Nelen A, Pettersson-Kymmer U, Eriksson S, Brenner H, Schöttker B, Saum KU, Holleczek B, Grodstein FD, Feskanich D, Orsini N, Wolk A, Bellavia A, Wilsgaard T, Jørgensen L, Boffetta P, Trichopoulos D, Trichopoulou A. Burden of hip fracture using disability-adjusted life-ye...
-
[6]
Webster J, Oguzman E, Morris EJA, Shepperd S, Griffin XL, Johansen A, Goldacre R. Trends and variation in the incidence of hip fracture in England before, during, and after the COVID -19 pandemic (2014-2024): a population-based observational study. Lancet Reg Health Eur. 2025;57:101427. Epub 20250813. doi: 10.1016/j.lanepe.2025.101427. PubMed PMID: 408372...
-
[7]
Updated practice guideline for dual-energy X-ray absorptiometry (DXA)
Slart R, Punda M, Ali DS, Bazzocchi A, Bock O, Camacho P, Carey JJ, Colquhoun A, Compston J, Engelke K, Erba PA, Harvey NC, Krueger D, Lems WF, Lewiecki EM, Morgan S, Moseley KF, O'Brien C, Probyn L, Rhee Y, Richmond B, Schousboe JT, Shuhart C, Ward KA, Van den Wyngaert T, Zhang -Yin J, Khan AA. Updated practice guideline for dual-energy X-ray absorptiome...
-
[8]
The clinician's guide to prevention and treatment of osteoporosis
LeBoff MS, Greenspan SL, Insogna KL, Lewiecki EM, Saag KG, Singer AJ, Siris ES. The clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int. 2022;33(10):2049 –102. Epub 20220428. doi: 10.1007/s00198-021-05900-y. PubMed PMID: 35478046; PubMed Central PMCID: PMC9546973
-
[9]
Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, Doubeni CA, Epling JW, Jr., Kemper AR, Kubik M, Landefeld CS, Mangione CM, Phipps MG, Pignone M, Silverstein M, Simon MA, Tseng CW, Wong JB. Screening for Osteoporosis to Prevent Fractures: US Preventive Services Task Force Recommendation Statement. Jama. 2018;319(24):2521–31. doi: 10.1001/j...
-
[10]
Osteopenia: a key target for fracture prevention
Reid IR, McClung MR. Osteopenia: a key target for fracture prevention. Lancet Diabetes Endocrinol. 2024;12(11):856–64. Epub 20240923. doi: 10.1016/s2213-8587(24)00225-0. PubMed PMID: 39326428
-
[11]
An overview of the use of the fracture risk assessment tool (FRAX) in osteoporosis
Schini M, Johansson H, Harvey NC, Lorentzon M, Kanis JA, McCloskey EV. An overview of the use of the fracture risk assessment tool (FRAX) in osteoporosis. J Endocrinol Invest. 2024;47(3):501 –
2024
-
[12]
doi: 10.1007/s40618-023-02219-9
Epub 20231024. doi: 10.1007/s40618-023-02219-9. PubMed PMID: 37874461; PubMed Central PMCID: PMC10904566
-
[13]
The UK Biobank resource with deep phenotyping and genomic data
Bycroft C, Freeman C, Petkova D, Band G, Elliott LT, Sharp K, Motyer A, Vukcevic D, Delaneau O, O'Connell J, Cortes A, Welsh S, Young A, Effingham M, McVean G, Leslie S, Allen N, Donnelly P, Marchini J. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562(7726):203–9. Epub 20181010. doi: 10.1038/s41586-018-0579-z. PubMed PMID: ...
-
[14]
Wu Y, Chao J, Bao M, Zhang N. Predictive value of machine learning on fracture risk in osteoporosis: a systematic review and meta-analysis. BMJ Open. 2023;13(12):e071430. Epub 20231209. doi: 10.1136/bmjopen-2022-071430. PubMed PMID: 38070927; PubMed Central PMCID: PMC10728980
-
[15]
Qian Y, Xia J, Liu KQ, Xu L, Xie SY, Chen GB, Cong PK, Khederzadeh S, Zheng HF. Observational and genetic evidence highlight the association of human sleep behaviors with the incidence of fracture. Commun Biol. 2021;4(1):1339. Epub 20211126. doi: 10.1038/s42003 -021-02861-0. PubMed PMID: 34837057; PubMed Central PMCID: PMC8626439
-
[16]
Kim Y, Kim YG, Park JW, Kim BW, Shin Y, Kong SH, Kim JH, Lee YK, Kim SW, Shin CS. A CT - based Deep Learning Model for Predicting Subsequent Fracture Risk in Patients with Hip Fracture. Radiology. 2024;310(1):e230614. doi: 10.1148/radiol.230614. PubMed PMID: 38289213
-
[17]
Machine Learning-Based CT Radiomics Model to Predict the Risk of Hip Fragility Fracture
Yuan J, Li B, Zhang C, Wang J, Huang B, Ma L. Machine Learning-Based CT Radiomics Model to Predict the Risk of Hip Fragility Fracture. Acad Radiol. 2025;32(5):2854–62. Epub 20250203. doi: 10.1016/j.acra.2025.01.023. PubMed PMID: 39904664
-
[18]
Nethander M, Coward E, Reimann E, Grahnemo L, Gabrielsen ME, Wibom C, Mägi R, Funck - Brentano T, Hoff M, Langhammer A, Pettersson-Kymmer U, Hveem K, Ohlsson C. Assessment of the genetic and clinical determinants of hip fracture risk: Genome-wide association and Mendelian randomization study. Cell Rep Med. 2022;3(10):100776. doi: 10.1016/j.xcrm.2022.10077...
-
[19]
Ito C, Al-Hassany L, Kurth T, Glatz T. Distinguishing Description, Prediction, and Causal Inference: A Primer on Improving Congruence Between Research Questions and Methods. Neurology. 2025;104(4):e210171. Epub 20250203. doi: 10.1212/wnl.0000000000210171. PubMed PMID: 39899793
-
[20]
Dyer BP. The distinction between causal, predictive, and descriptive research -there is still room for improvement. J Clin Epidemiol. 2026;189:111960. Epub 20250901. doi: 10.1016/j.jclinepi.2025.111960. PubMed PMID: 40902863
-
[21]
Morin SN, Leslie WD, Schousboe JT. Osteoporosis: A Review. Jama. 2025;334(10):894 –907. doi: 10.1001/jama.2025.6003. PubMed PMID: 40587168
-
[22]
Causal Inference About the Effects of Interventions From Observational Studies in Medical Journals
Dahabreh IJ, Bibbins-Domingo K. Causal Inference About the Effects of Interventions From Observational Studies in Medical Journals. Jama. 2024;331(21):1845 –53. doi: 10.1001/jama.2024.7741. PubMed PMID: 38722735
-
[23]
Confounder Selection in Observational Studies in High-Impact Medical and Epidemiological Journals
Correia LCL, Mascarenhas RF, De Menezes FSC, Oliveira JSJ, Vaccarino V, Ross JS, Wallach JD. Confounder Selection in Observational Studies in High-Impact Medical and Epidemiological Journals. JAMA Netw Open. 2025;8(7):e2524176. Epub 20250701. doi: 10.1001/jamanetworkopen.2025.24176. PubMed PMID: 40711790
-
[24]
Aga R, Søgaard AJ, Holvik K, Hagen TP, Idland G, Jeyananthan A, Melhuus KR, Rognerud M, Samuelsen SO, Meyer HE. Effectiveness of a fall and fracture prevention pathway on hip fracture risk, need of permanent care and mortality: a controlled before-and-after study. Age Ageing. 2025;54(6). doi: 10.1093/ageing/afaf161. PubMed PMID: 40552367; PubMed Central P...
-
[25]
Mann HB, Whitney DR. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. The Annals of Mathematical Statistics. 1947;18(1):50 –60. doi: 10.1214/aoms/1177730491
-
[26]
Pearson K. X. On the Criterion That a Given System of Deviations from the Probable in the Case of a Correlated System of Variables Is Such That It Can Be Reasonably Supposed to Have Arisen from Random Sampling. The London, Edinburgh, and Dublin Philosophical Magazine and Journal of Science. 1900;50(302):157–75. doi: 10.1080/14786440009463897
-
[27]
On the Interpretation of chi-square from Contingency Tables, and the Calculation of P
Fisher RA. On the Interpretation of chi-square from Contingency Tables, and the Calculation of P. Journal of the Royal Statistical Society. 1922;85(1):87–94. doi: 10.2307/2340521
-
[28]
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–107. doi: 10.1002/sim.3697. PubMed PMID: 19757444; PubMed Central PMCID: PMC3472075
-
[29]
How to use directed acyclic graphs: guide for clinical researchers
Feeney T, Hartwig FP, Davies NM. How to use directed acyclic graphs: guide for clinical researchers. Bmj. 2025;388:e078226. Epub 20250321. doi: 10.1136/bmj -2023-078226. PubMed PMID: 40118502
work page doi:10.1136/bmj 2025
-
[30]
Jepsen KJ, Bredbenner TL, Karvonen-Gutierrez CA, Leis AM, Hood MM, Harlow SD, Randolph J, Clines GA, Merillat S, Elliott MR, Cauley JA, Greendale GA, Karlamangla AS, Peters KW, Harrison SL, Lui LY, Cawthon PM, Orwoll E. Femoral neck width is associated with unique trajectories of age - related hip structural changes and fracture risk within populations of...
-
[31]
Hip Fracture Risk Assessment Tools for Adults Aged 80 Years and Older
Ensrud KE, Schousboe JT, Crandall CJ, Leslie WD, Fink HA, Cawthon PM, Kado DM, Lane NE, Cauley JA, Langsetmo L. Hip Fracture Risk Assessment Tools for Adults Aged 80 Years and Older. JAMA Netw Open. 2024;7(6):e2418612. Epub 20240603. doi: 10.1001/jamanetworkopen.2024.18612. PubMed PMID: 38941095; PubMed Central PMCID: PMC11214124
-
[32]
Sex differences in the spatial distribution of bone in relation to incident hip fracture: Findings from the AGES-Reykjavik study
Marques EA, Carballido-Gamio J, Gudnason V, Sigurdsson G, Sigurdsson S, Aspelund T, Siggeirsdottir K, Launer L, Eiriksdottir G, Lang T, Harris TB. Sex differences in the spatial distribution of bone in relation to incident hip fracture: Findings from the AGES-Reykjavik study. Bone. 2018;114:72–
2018
-
[33]
doi: 10.1016/j.bone.2018.05.016
Epub 20180516. doi: 10.1016/j.bone.2018.05.016. PubMed PMID: 29777918; PubMed Central PMCID: PMC6137723
-
[34]
Scaling of adult human bone and skeletal muscle mass to height in the US population
Heymsfield SB, Hwaung P, Ferreyro-Bravo F, Heo M, Thomas DM, Schuna JM, Jr. Scaling of adult human bone and skeletal muscle mass to height in the US population. Am J Hum Biol. 2019;31(4):e23252. Epub 20190514. doi: 10.1002/ajhb.23252. PubMed PMID: 31087593; PubMed Central PMCID: PMC6634976
-
[35]
Height and Risk of Hip Fracture: A Meta - Analysis of Prospective Cohort Studies
Xiao Z, Ren D, Feng W, Chen Y, Kan W, Xing D. Height and Risk of Hip Fracture: A Meta - Analysis of Prospective Cohort Studies. Biomed Res Int. 2016;2016:2480693. Epub 20161012. doi: 10.1155/2016/2480693. PubMed PMID: 27818998; PubMed Central PMCID: PMC5080474
-
[36]
Obesity is associated with early hip fracture risk in postmenopausal women: a 25-year follow-up
Rikkonen T, Sund R, Sirola J, Honkanen R, Poole KES, Kröger H. Obesity is associated with early hip fracture risk in postmenopausal women: a 25-year follow-up. Osteoporos Int. 2021;32(4):769–77. Epub 20201023. doi: 10.1007/s00198-020-05665-w. PubMed PMID: 33095419; PubMed Central PMCID: PMC8026440
-
[37]
Amin H, Khan MA, Bukhari M. Deprivation indices and their association with fragility fractures and bone density: evidence from a large observational cohort. Rheumatology (Oxford). 2026;65(1). doi: 10.1093/rheumatology/keaf550. PubMed PMID: 41105243; PubMed Central PMCID: PMC12862389
-
[38]
Li H, Wallin M, Barregard L, Sallsten G, Lundh T, Ohlsson C, Mellström D, Andersson EM. Smoking-Induced Risk of Osteoporosis Is Partly Mediated by Cadmium From Tobacco Smoke: The MrOS Sweden Study. J Bone Miner Res. 2020;35(8):1424–9. Epub 20200406. doi: 10.1002/jbmr.4014. PubMed PMID: 32191351
-
[39]
Zoulakis M, Ambjörn M, Jaiswal R, Axelsson KF, Litsne H, Johansson L, Lorentzon M. Impact of Current and Previous Smoking on Fracture Risk in Older Women: The Role of Physical Function, Bone Density and Bone Microarchitecture. J Bone Miner Res. 2026. Epub 20260210. doi: 10.1093/jbmr/zjag028. PubMed PMID: 41665281
-
[40]
Godos J, Giampieri F, Chisari E, Micek A, Paladino N, Forbes-Hernández TY, Quiles JL, Battino M, La Vignera S, Musumeci G, Grosso G. Alcohol Consumption, Bone Mineral Density, and Risk of Osteoporotic Fractures: A Dose-Response Meta-Analysis. Int J Environ Res Public Health. 2022;19(3). Epub 20220128. doi: 10.3390/ijerph19031515. PubMed PMID: 35162537; Pu...
-
[41]
Denova-Gutiérrez E, Méndez-Sánchez L, Muñoz-Aguirre P, Tucker KL, Clark P. Dietary Patterns, Bone Mineral Density, and Risk of Fractures: A Systematic Review and Meta -Analysis. Nutrients. 2018;10(12). Epub 20181205. doi: 10.3390/nu10121922. PubMed PMID: 30563066; PubMed Central PMCID: PMC6316557
-
[42]
Bone mineral density status in patients with recent-onset rheumatoid arthritis
Ketabforoush A, Aleahmad M, Qorbani M, Mehrpoor G, Afrashteh S, Mardi S, Dolatshahi E. Bone mineral density status in patients with recent-onset rheumatoid arthritis. J Diabetes Metab Disord. 2023;22(1):775–85. Epub 20230317. doi: 10.1007/s40200-023-01200-w. PubMed PMID: 37250372; PubMed Central PMCID: PMC10023217
-
[43]
Rheumatoid arthritis and subsequent fracture risk: an individual person meta-analysis to update FRAX
Kanis JA, Johansson H, McCloskey EV, Liu E, Schini M, Vandenput L, Åkesson KE, Anderson FA, Azagra R, Bager CL, Beaudart C, Bischoff-Ferrari HA, Biver E, Bruyère O, Cauley JA, Center JR, Chapurlat R, Christiansen C, Cooper C, Crandall CJ, Cummings SR, da Silva JAP, Dawson -Hughes B, Diez-Perez A, Dufour AB, Eisman JA, Elders PJM, Ferrari S, Fujita Y, Fuji...
-
[44]
Leslie WD, Lix LM, Binkley N. Osteoporosis treatment considerations based upon fracture history, fracture risk assessment, vertebral fracture assessment, and bone density in Canada. Arch Osteoporos. 2020;15(1):93. Epub 20200623. doi: 10.1007/s11657-020-00775-8. PubMed PMID: 32577922
-
[45]
Hu Q, Liu H, Du Y, Duan R, Li L, Yang D, Ouyang Z. Walking pace and its association with osteoporosis and pathological fractures: insights from UK biobank. Front Endocrinol (Lausanne). 2025;16:1635999. Epub 20250826. doi: 10.3389/fendo.2025.1635999. PubMed PMID: 40933376; PubMed Central PMCID: PMC12417151
-
[46]
Huang SG, Lee RP, Yao TK, Wang JH, Wu WT, Yeh KT. Correlation Between Handgrip Strength and Bone Density and Fragility Fracture Risk Among Older Adults: A Cross -Sectional Study. J Nurs Res. 2025;33(1):e375. Epub 20250201. doi: 10.1097/jnr.0000000000000656. PubMed PMID: 39835766
-
[47]
Causal Inference: What If
Hernán MA, Robins JM. Causal Inference: What If. Boca Raton: Chapman & Hall/CRC; 2020
2020
-
[48]
Causality: Models, Reasoning, and Inference
Pearl J. Causality: Models, Reasoning, and Inference. 2nd ed: Cambridge University Press; 2009
2009
-
[49]
Athey S, Tibshirani J, Wager S. Generalized Random Forests. The Annals of Statistics. 2019;47(2):1148–78. doi: 10.1214/18-AOS1709
-
[50]
Journal of the American Statistical Association , author =
Wager S, Athey S. Estimation and Inference of Heterogeneous Treatment Effects using Random Forests. Journal of the American Statistical Association. 2018;113(523):1228 –42. doi: 10.1080/01621459.2017.1319839
-
[51]
Hsieh CI, Zheng K, Lin C, Mei L, Lu L, Li W, Chen FP, Wang Y, Zhou X, Wang F, Xie G, Xiao J, Miao S, Kuo CF. Automated bone mineral density prediction and fracture risk assessment using plain radiographs via deep learning. Nat Commun. 2021;12(1):5472. Epub 20210916. doi: 10.1038/s41467 - 021-25779-x. PubMed PMID: 34531406; PubMed Central PMCID: PMC8446034
-
[52]
Jaiswal R, Pivodic A, Zoulakis M, Axelsson KF, Litsne H, Johansson L, Lorentzon M. Prediction of hip fracture by high-resolution peripheral quantitative computed tomography in older Swedish women. J Bone Miner Res. 2025;40(6):779–90. doi: 10.1093/jbmr/zjaf020. PubMed PMID: 39869791; PubMed Central PMCID: PMC12131241
-
[53]
Femoral neck width genetic risk score is a novel independent risk factor for hip fractures
Tobias JH, Nethander M, Faber BG, Heppenstall SV, Ebsim R, Cootes T, Lindner C, Saunders FR, Gregory JS, Aspden RM, Harvey NC, Kemp JP, Frysz M, Ohlsson C. Femoral neck width genetic risk score is a novel independent risk factor for hip fractures. J Bone Miner Res. 2024;39(3):241 –51. doi: 10.1093/jbmr/zjae002. PubMed PMID: 38477772; PubMed Central PMCID:...
-
[54]
Metalearners for estimating heterogeneous treatment effects using machine learning
Künzel SR, Sekhon JS, Bickel PJ, Yu B. Metalearners for estimating heterogeneous treatment effects using machine learning. Proc Natl Acad Sci U S A. 2019;116(10):4156 –65. Epub 20190215. doi: 10.1073/pnas.1804597116. PubMed PMID: 30770453; PubMed Central PMCID: PMC6410831
-
[55]
Khan AA, Slart R, Ali DS, Bock O, Carey JJ, Camacho P, Engelke K, Erba PA, Harvey NC, Lems WF, Morgan S, Moseley KF, O'Brien C, Probyn L, Punda M, Richmond B, Schousboe JT, Shuhart C, Ward KA, Lewiecki EM. Osteoporotic Fractures: Diagnosis, Evaluation, and Significance From the International Working Group on DXA Best Practices. Mayo Clin Proc. 2024;99(7):...
-
[56]
A Unified Approach to Interpreting Model Predictions
Lundberg SM, Lee S-I, editors. A Unified Approach to Interpreting Model Predictions. Advances in Neural Information Processing Systems; 2017: Curran Associates, Inc
2017
-
[57]
Li GH, Cheung CL, Tan KC, Kung AW, Kwok TC, Lau WC, Wong JS, Hsu WWQ, Fang C, Wong IC. Development and validation of sex-specific hip fracture prediction models using electronic health records: a retrospective, population-based cohort study. EClinicalMedicine. 2023;58:101876. Epub 20230227. doi: 10.1016/j.eclinm.2023.101876. PubMed PMID: 36896245; PubMed ...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.