Establishing the Minimal Clinically Important Difference (MCID) for Smartphone-Derived Gait Measures in Multiple Sclerosis
Pith reviewed 2026-06-30 01:25 UTC · model grok-4.3
The pith
Smartphone gait measures in progressive MS have triangulated MCIDs of -0.16 m/s step velocity, 0.06 s step duration, and similar values for other metrics.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
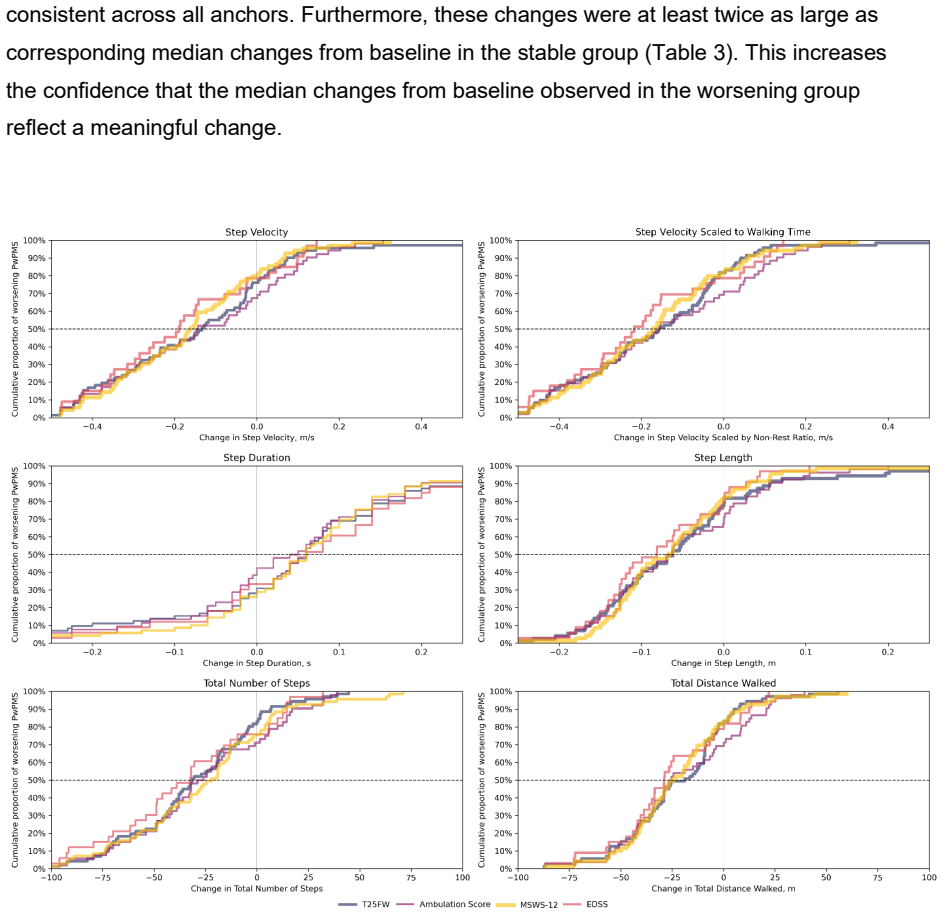
Using data from 243 patients, median changes from baseline at Week 96 on digital gait measures were computed for those showing clinically meaningful worsening on the Timed 25-Foot Walk, Ambulation Score, Expanded Disability Status Scale, or 12-item Multiple Sclerosis Walking Scale; triangulation of these changes yields MCIDs of Step Velocity = -0.16 m/s, Step Velocity Scaled to Walking Time = -0.18 m/s, Step Duration = 0.06 s, Step Length = -0.07 m, Total Number of Steps = -28, and Total Distance Walked = -24 m.
What carries the argument
Anchor-based triangulation of median gait changes observed in the subgroup of patients worsening on any of four clinical anchors.
If this is right
- These MCIDs allow longitudinal smartphone data to flag meaningful worsening rather than normal fluctuation.
- Digital gait endpoints in future MS trials can use the thresholds to assess treatment effects.
- Remote monitoring gains an objective basis for detecting progression between clinic visits.
- Personalized care plans can incorporate frequent gait tracking with interpretable change criteria.
Where Pith is reading between the lines
- Independent validation in relapsing-remitting MS or other gait disorders would test generalizability of the thresholds.
- Frequent remote testing enabled by these MCIDs could detect progression earlier than infrequent in-clinic assessments.
- Integration with other digital biomarkers might increase sensitivity for tracking disease course.
Load-bearing premise
The four clinical anchors validly identify patients with clinically meaningful worsening, and the median digital gait changes in that subgroup equal the minimal important difference.
What would settle it
A replication study that applies the same four anchors to a comparable progressive MS cohort and finds median gait changes at the corresponding time point differing substantially from the reported values would falsify the MCIDs.
Figures
read the original abstract
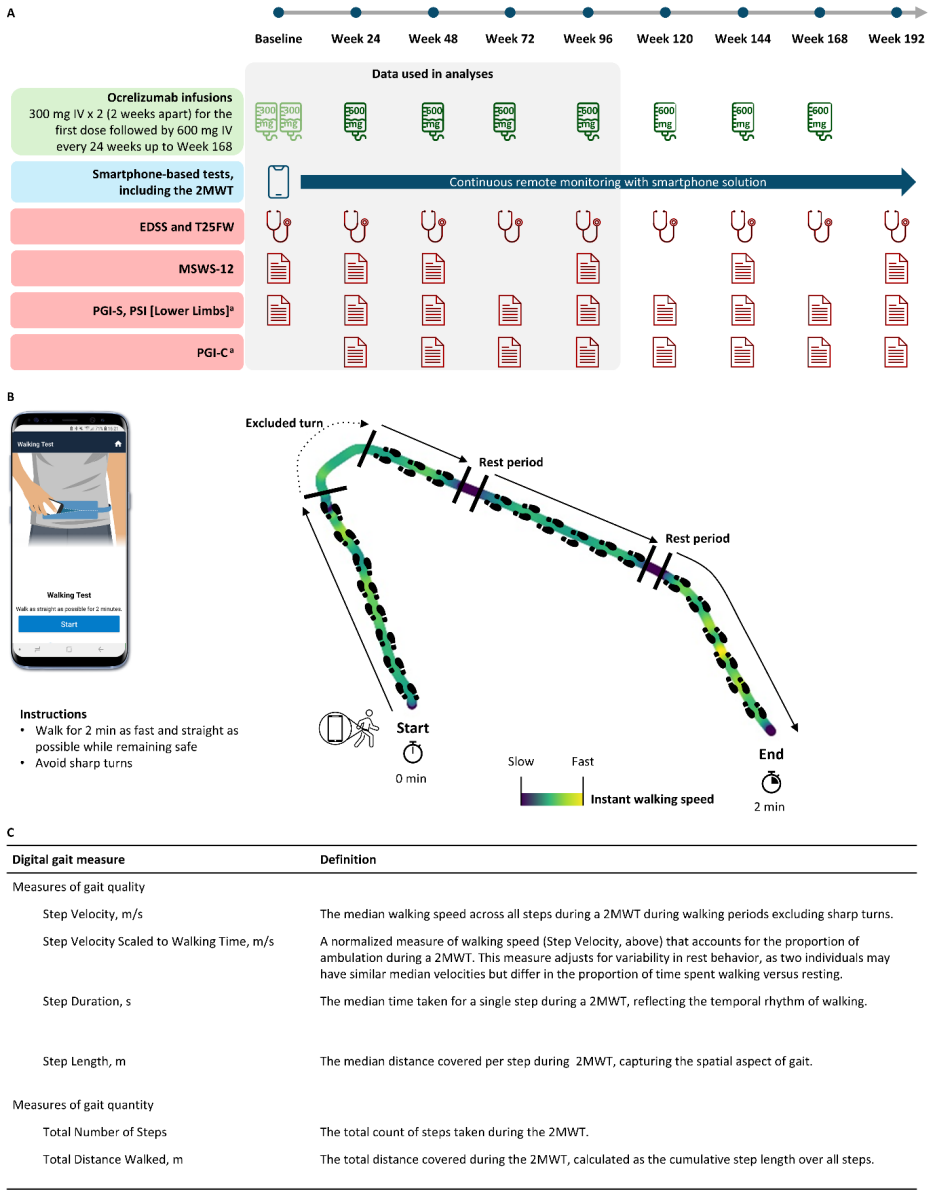
Background: Digital health technologies allow for frequent, remote gait monitoring in people with multiple sclerosis (MS). However, to differentiate daily variability from actual disease progression in longitudinal data, established minimal clinically important differences (MCID) are required. Currently, there is limited literature defining these thresholds for digital gait metrics. Objective: To establish MCIDs for digital gait measures reflecting progression in MS. Methods: Digital gait measures were captured via daily, remote, smartphone-based Two-Minute Walk Tests in CONSONANCE (NCT03523858), a phase 3b study of ocrelizumab in progressive MS. Using an anchor-based approach, median changes from baseline at Week 96 on digital gait measures were computed for patients showing clinically meaningful worsening on either Timed 25-Foot Walk, Ambulation Score, Expanded Disability Status Scale, or 12-item Multiple Sclerosis Walking Scale. These changes were subsequently triangulated to derive the MCID estimates. Results: 243 patients with progressive MS (female: n=125 (51%); mean [SD] age: 49.3 [9.3]; mean [SD] EDSS: 4.8 [1.4]) had digital gait data available at baseline and Week 96. Median changes were generally consistent across anchors. Triangulated MCIDs are: Step Velocity = -0.16 m/s, Step Velocity Scaled to Walking Time = -0.18 m/s, Step Duration = 0.06 s, Step Length = -0.07 m, Total Number of Steps = -28, and Total Distance Walked = -24 m. Conclusion: These MCIDs provide a framework for interpreting meaningful gait changes and integrating digital measures into MS outcome evaluation. Beyond facilitating novel clinical trial endpoints to evaluate treatment efficacy, they enable objective, real-world monitoring to advance personalized patient care.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript claims to establish MCIDs for six smartphone-derived gait measures (step velocity, step velocity scaled to walking time, step duration, step length, total steps, total distance) in progressive MS via an anchor-based triangulation. Using daily remote 2MWT data from 243 patients in the CONSONANCE trial, the authors compute median changes from baseline to Week 96 among those showing worsening on at least one of four clinical anchors (T25FW, Ambulation Score, EDSS, MSWS-12) and triangulate these to obtain the reported thresholds (e.g., -0.16 m/s for step velocity).
Significance. If the anchor-based medians are shown to be robust, the MCIDs would provide a practical framework for interpreting longitudinal digital gait data in MS, enabling differentiation of progression from variability and supporting both trial endpoints and real-world monitoring. The sample size and remote smartphone collection are strengths for applicability.
major comments (2)
- [Abstract/Methods] Abstract/Methods: The central derivation pools patients who worsen on any of the four anchors and equates the median digital-gait change in this subgroup directly to the MCID. No anchor–digital correlations, overlap statistics, or specificity of the 'worsening on ≥1' rule are reported, so it is unclear whether the resulting values (-0.16 m/s, -0.07 m, etc.) represent minimal clinically important thresholds or averages across heterogeneous subgroups.
- [Results] Results: The abstract states median changes were 'generally consistent across anchors' but provides no IQR, standard errors, or sensitivity analyses (e.g., requiring worsening on ≥2 anchors or restricting to gait-specific anchors). Without these, the triangulation step and the claim that the values are suitable for distinguishing progression remain insufficiently supported.
minor comments (1)
- [Abstract] Abstract: The triangulation procedure (how the anchor-specific medians are combined into the final MCID) is not described; a brief statement of the rule used would improve clarity.
Simulated Author's Rebuttal
We thank the referee for their constructive comments, which have helped us identify areas to strengthen the clarity and robustness of our MCID estimates. We respond to each major comment below.
read point-by-point responses
-
Referee: [Abstract/Methods] Abstract/Methods: The central derivation pools patients who worsen on any of the four anchors and equates the median digital-gait change in this subgroup directly to the MCID. No anchor–digital correlations, overlap statistics, or specificity of the 'worsening on ≥1' rule are reported, so it is unclear whether the resulting values (-0.16 m/s, -0.07 m, etc.) represent minimal clinically important thresholds or averages across heterogeneous subgroups.
Authors: The anchor-based MCID method we employed is standard in the literature, defining the MCID as the median change observed in patients who demonstrate worsening on established clinical anchors. The use of 'worsening on at least one anchor' captures patients with any form of clinical deterioration relevant to gait. While we did not report correlations or overlap statistics in the original submission, these can be computed from the available data. We will add Spearman correlations between the digital gait measures and the anchors, as well as the distribution of patients worsening on one versus multiple anchors, to a revised manuscript. This will help demonstrate the specificity and support the triangulation approach. revision: yes
-
Referee: [Results] Results: The abstract states median changes were 'generally consistent across anchors' but provides no IQR, standard errors, or sensitivity analyses (e.g., requiring worsening on ≥2 anchors or restricting to gait-specific anchors). Without these, the triangulation step and the claim that the values are suitable for distinguishing progression remain insufficiently supported.
Authors: We agree that additional details on variability and sensitivity would enhance the support for our findings. In the revised manuscript, we will report the interquartile ranges and, where appropriate, standard errors for the median changes stratified by each anchor. Furthermore, we will conduct and present sensitivity analyses, including those requiring worsening on at least two anchors and those limited to gait-specific anchors (T25FW, Ambulation Score, and MSWS-12). These additions will be included in the Results section and a new supplementary table to better substantiate the triangulation and the applicability of the MCIDs for distinguishing progression. revision: yes
Circularity Check
No circularity; MCIDs derived empirically from external clinical anchors
full rationale
The derivation selects patients worsening on independent external anchors (T25FW, Ambulation Score, EDSS, MSWS-12), computes observed median changes in digital gait metrics within that subgroup at Week 96, and triangulates those medians. This is a direct empirical calculation from data; no equation reduces the MCID values to a fitted parameter, self-referential definition, or self-citation chain. The anchors are not derived from the digital measures, and no uniqueness theorem or ansatz is imported. The result is self-contained against external benchmarks and receives a normal non-finding.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Clinical anchors (T25FW, Ambulation Score, EDSS, MSWS-12) accurately identify patients with clinically meaningful worsening
Reference graph
Works this paper leans on
-
[1]
Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018;391:1622–1636. Available at: https://doi.org/10.1016/S0140-6736(18)30481-1
-
[2]
New insights into the burden and costs of multiple sclerosis in Europe
Kobelt G, Thompson A, Berg J, Gannedahl M, Eriksson J. New insights into the burden and costs of multiple sclerosis in Europe. Mult. Scler. J. 2017;23:1123–1136
2017
-
[3]
The impact of slower walking speed on activities of daily living in patients with multiple sclerosis
Yildiz M. The impact of slower walking speed on activities of daily living in patients with multiple sclerosis. Int. J. Clin. Pr. 2012;66:1088–1094. Available at: https://doi.org/10.1111/ijcp.12003
-
[4]
Gait deficits in people with multiple sclerosis: A systematic review and meta-analysis
Comber L, Galvin R, Coote S. Gait deficits in people with multiple sclerosis: A systematic review and meta-analysis. Gait Posture. 2017;51:25–35
2017
-
[5]
Impact of Walking Impairment in Multiple Sclerosis
LaRocca NG. Impact of Walking Impairment in Multiple Sclerosis. Patient: Patient- Centered Outcomes Res. 2011;4:189–201. Available at: https://doi.org/10.2165/11591150- 000000000-00000
-
[6]
Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable
Heesen C, Böhm J, Reich C, Kasper J, Goebel M, Gold S. Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable. Mult Scler. 2008;14:988–991
2008
-
[7]
Time between expanded disability status scale (EDSS) scores
Zurawski J, Glanz BI, Chua A, et al. Time between expanded disability status scale (EDSS) scores. Mult. Scler. Relat. Disord. 2019;30:98–103. 28
2019
-
[8]
I have to walk a lot slower, and I seem to sometimes have to almost limp a little bit
Griffiths P, Sims J, Williams A, et al. How strong should my anchor be for estimating group and individual level meaningful change? A simulation study assessing anchor correlation strength and the impact of sample size, distribution of change scores and methodology on establishing a true meaningful change threshold. Quality of life research : an internati...
2023
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.