Anatomically Consistent TMJ Disc Segmentation via Semantic Anchoring and Clinical Priors
Pith reviewed 2026-06-26 12:59 UTC · model grok-4.3
The pith
A new framework combines semantic anchoring in foundation-model features with mouth-open-limitation metadata to produce more anatomically consistent TMJ disc segmentations from MRI.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
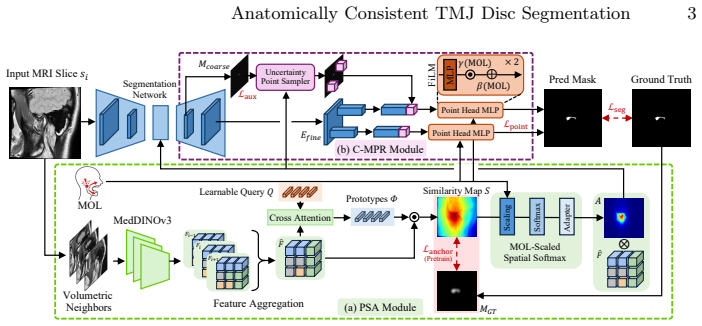
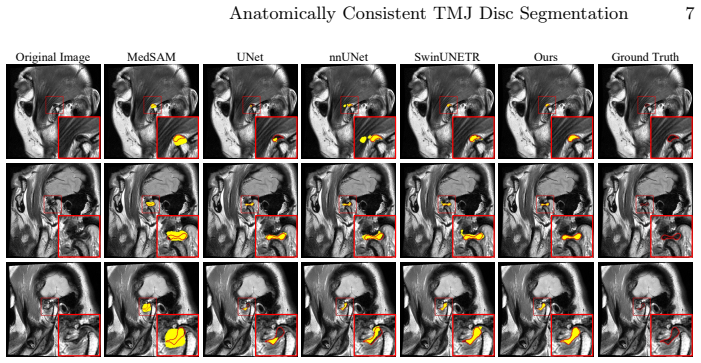
TISC establishes robust disc localization in foundation-model feature space through a Prototypical Semantic Anchoring module that aggregates adjacent-slice MedDINOv3 features into a prototype-driven similarity map, then performs targeted boundary refinement via a Clinical-Metadata Point Refinement module whose point-wise predictions are modulated by the Mouth Open Limitation clinical indicator, delivering up to 4.96 Dice improvement and more coherent masks across diverse architectures on a cohort of 2,488 PD MRI volumes from 1,300 patients.
What carries the argument
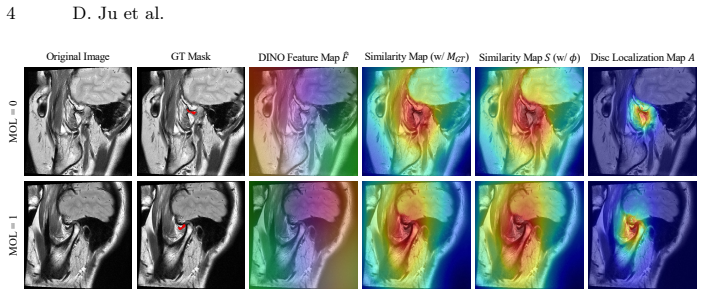
The Prototypical Semantic Anchoring (PSA) module aggregates adjacent-slice MedDINOv3 features to create a prototype-driven similarity map for initial disc localization, paired with the Clinical-Metadata Point Refinement (C-MPR) module that adjusts point predictions using Mouth Open Limitation metadata.
If this is right
- Downstream measurements of disc position and shape become more stable for diagnosis of internal derangement.
- Fragmented or anatomically inconsistent masks are reduced across multiple segmentation backbones.
- Clinical metadata can be used as a lightweight prior to improve boundary accuracy without retraining the entire model.
- The approach scales to large patient cohorts while remaining compatible with existing foundation-model features.
Where Pith is reading between the lines
- The same anchoring-plus-metadata pattern could be tested on other small low-contrast anatomical structures where limited clinical indicators exist.
- If foundation-model features already encode enough semantic structure, the need for task-specific annotated data may decrease when clinical priors are added.
- Performance on different MRI field strengths or sequences would test whether the prototype similarity map generalizes beyond the training distribution.
Load-bearing premise
The Clinical-Metadata Point Refinement module assumes Mouth Open Limitation clinical data is both available and causally informative for modulating boundary predictions without introducing systematic errors from missing or inaccurate metadata.
What would settle it
A blinded comparison of the same images segmented with and without accurate Mouth Open Limitation metadata, or on a held-out cohort where the metadata is withheld or deliberately corrupted, would show whether the refinement step measurably improves coherence or instead adds bias.
Figures
read the original abstract
Segmenting the temporomandibular joint (TMJ) disc from MRI is essential for accurate diagnosis of internal derangement, yet it remains unreliable in practice due to its small size, low contrast, and morphological variability. Existing methods, primarily adapted from general segmentation architectures, often produce fragmented or anatomically inconsistent masks, leading to unstable measurements of disc position and shape for downstream diagnosis. To address these challenges, we propose TISC, a TMJ disc segmentation framework that integrates semantic anchoring with clinical metadata-guided boundary refinement. The framework first establishes robust disc localization in the foundation model feature space via a Prototypical Semantic Anchoring (PSA) module that aggregates adjacent-slice MedDINOv3 features and derives a prototype-driven similarity map. It then performs targeted boundary refinement through a Clinical-Metadata Point Refinement (C-MPR) module, with point-wise predictions modulated by Mouth Open Limitation (MOL), a clinical indicator associated with disc displacement without reduction. On a large-scale cohort of 2,488 PD MRI volumes from 1,300 patients, our method achieves up to a 4.96 Dice improvement over strong baselines across diverse architectures, delivering more anatomically coherent and clinically reliable TMJ disc segmentation.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes TISC, a TMJ disc segmentation framework that combines a Prototypical Semantic Anchoring (PSA) module for localizing the disc via aggregated MedDINOv3 features from adjacent slices and a Clinical-Metadata Point Refinement (C-MPR) module that modulates point-wise boundary predictions using Mouth Open Limitation (MOL) clinical metadata. On a cohort of 2,488 PD MRI volumes from 1,300 patients, the method is reported to achieve up to a 4.96 Dice improvement over strong baselines across diverse architectures while producing more anatomically coherent segmentations.
Significance. If the reported gains are substantiated by complete experimental protocols, ablations, and robustness checks, the incorporation of clinical priors such as MOL into segmentation could meaningfully improve anatomical consistency and downstream diagnostic utility for TMJ internal derangement. The scale of the cohort is a positive factor, but the absence of supporting validation details limits the immediate impact assessment.
major comments (2)
- [C-MPR module description and experimental results] The central performance claim (up to 4.96 Dice gain) is attributed in part to the C-MPR module's modulation of predictions by MOL values. No ablation on MOL-missing subsets, sensitivity analysis to MOL measurement noise, or patient-level split statistics confirming no leakage are provided, directly undercutting the assertion of 'clinically reliable' results in real-world settings where metadata completeness varies.
- [Abstract and Experiments section] The abstract and method summary state numerical improvements and name the two modules but supply no experimental protocol, statistical tests (e.g., paired t-tests or Wilcoxon), ablation results isolating PSA vs. C-MPR contributions, or error analysis (e.g., failure cases by disc morphology). This prevents evaluation of whether the gains are robust or artifactual.
minor comments (1)
- [Method] Notation for the prototype-driven similarity map and point-wise modulation in PSA and C-MPR should be formalized with equations to allow reproducibility.
Simulated Author's Rebuttal
We thank the referee for the constructive comments regarding validation rigor and experimental transparency. We address each major comment point by point below, clarifying existing content in the manuscript and indicating revisions where additional analyses will strengthen the claims.
read point-by-point responses
-
Referee: [C-MPR module description and experimental results] The central performance claim (up to 4.96 Dice gain) is attributed in part to the C-MPR module's modulation of predictions by MOL values. No ablation on MOL-missing subsets, sensitivity analysis to MOL measurement noise, or patient-level split statistics confirming no leakage are provided, directly undercutting the assertion of 'clinically reliable' results in real-world settings where metadata completeness varies.
Authors: We agree these additional checks would better support real-world applicability. The cohort of 2,488 volumes from 1,300 patients was acquired under a standardized clinical protocol that recorded MOL for every case, and all experiments used patient-level partitioning to prevent leakage (detailed in Section 4.1 with patient counts per fold). To directly address the concern, the revised manuscript will add: (1) an ablation simulating MOL-missing subsets via random masking, (2) sensitivity analysis introducing controlled noise to MOL values, and (3) explicit patient-level split statistics. These will be presented as new experiments supporting the clinical reliability claim. revision: yes
-
Referee: [Abstract and Experiments section] The abstract and method summary state numerical improvements and name the two modules but supply no experimental protocol, statistical tests (e.g., paired t-tests or Wilcoxon), ablation results isolating PSA vs. C-MPR contributions, or error analysis (e.g., failure cases by disc morphology). This prevents evaluation of whether the gains are robust or artifactual.
Authors: The Experiments section (Section 4) details the full protocol, including 5-fold patient-level cross-validation, implementation of baselines across architectures, and Dice scores with standard deviations. Ablations isolating PSA and C-MPR contributions appear in Table 3, while paired t-tests with p-values are reported for significance. We will revise the abstract to briefly reference the evaluation protocol and add a dedicated error analysis subsection stratifying failures by disc morphology categories. These changes will be incorporated in the revised version. revision: partial
Circularity Check
No circularity: purely empirical method with no derivations
full rationale
The paper describes an empirical TMJ disc segmentation framework (TISC) consisting of PSA and C-MPR modules, evaluated via Dice scores on an external cohort of 2488 PD MRI volumes. No equations, first-principles derivations, uniqueness theorems, or predictions that reduce to fitted inputs are presented anywhere in the provided text. Performance claims rest on direct measurement against baselines rather than any self-referential construction, self-citation load-bearing argument, or ansatz smuggled via prior work. The reader's assessment of score 1.0 is consistent with the absence of any load-bearing mathematical chain.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption Adjacent-slice MedDINOv3 features can be aggregated into a prototype that reliably localizes the TMJ disc
- domain assumption Mouth Open Limitation is a valid clinical indicator that can modulate point-wise boundary predictions without introducing bias
Reference graph
Works this paper leans on
-
[1]
Association, W.M., et al.: World medical association declaration of helsinki: ethical principlesformedicalresearchinvolvinghumansubjects.Jama310(20),2191–2194 (2013)
2013
-
[2]
World journal of radi- ology6(8), 567 (2014)
Bag, A.K., Gaddikeri, S., Singhal, A., Hardin, S., Tran, B.D., Medina, J.A., Curé, J.K.: Imaging of the temporomandibular joint: An update. World journal of radi- ology6(8), 567 (2014)
2014
-
[3]
Dice,L.R.:Measuresoftheamountofecologicassociationbetweenspecies.Ecology 26(3), 297–302 (1945)
1945
-
[4]
In: International MICCAI brainlesion workshop
Hatamizadeh, A., Nath, V., Tang, Y., Yang, D., Roth, H.R., Xu, D.: Swin unetr: Swin transformers for semantic segmentation of brain tumors in mri images. In: International MICCAI brainlesion workshop. pp. 272–284. Springer (2021)
2021
-
[5]
In: WACV
Hatamizadeh, A., Tang, Y., Nath, V., Yang, D., Myronenko, A., Landman, B., Roth, H.R., Xu, D.: Unetr: Transformers for 3d medical image segmentation. In: WACV. pp. 574–584 (2022)
2022
-
[6]
He,K.,Zhang,X.,Ren,S.,Sun,J.:Deepresiduallearningforimagerecognition.In: Proceedings of the IEEE conference on computer vision and pattern recognition. pp. 770–778 (2016)
2016
-
[7]
Scientific Reports11(1), 20917 (2021)
Hegab, A.F., Al Hameed, H.I., Karam, K.S.: Classification of temporomandibu- lar joint internal derangement based on magnetic resonance imaging and clinical findings of 435 patients contributing to a nonsurgical treatment protocol. Scientific Reports11(1), 20917 (2021)
2021
-
[8]
arXiv preprint arXiv:1809.10486 (2018) 10 D
Isensee,F.,Petersen,J.,Klein,A.,Zimmerer,D.,Jaeger,P.F.,Kohl,S.,Wasserthal, J., Koehler, G., Norajitra, T., Wirkert, S., et al.: nnu-net: Self-adapting frame- work for u-net-based medical image segmentation. arXiv preprint arXiv:1809.10486 (2018) 10 D. Ju et al
Pith/arXiv arXiv 2018
-
[9]
Scientific Reports12(1), 221 (2022)
Ito, S., Mine, Y., Yoshimi, Y., Takeda, S., Tanaka, A., Onishi, A., Peng, T.Y., Nakamoto, T., Nagasaki, T., Kakimoto, N., et al.: Automated segmentation of articular disc of the temporomandibular joint on magnetic resonance images using deep learning. Scientific Reports12(1), 221 (2022)
2022
-
[10]
npj Digital Medicine (2026)
Jung, H.J., Ju, D., Kim, C., Hwang, S.J., Lee, C., Park, Y.: Multimodal deep learning with anatomically constrained attention for screening mri-detectable tmj abnormalities from panoramic images. npj Digital Medicine (2026)
2026
-
[11]
In: CVPR
Kirillov, A., Wu, Y., He, K., Girshick, R.: Pointrend: Image segmentation as ren- dering. In: CVPR. pp. 9799–9808 (2020)
2020
-
[12]
Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology90(1), 16–20 (2000)
Kurita, H., Ohtsuka, A., Kobayashi, H., Kurashina, K.: The relationship between the degree of disk displacement and ability to perform disk reduction. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology90(1), 16–20 (2000)
2000
-
[13]
Dentomaxillofacial Radiology44(1), 20140235 (2015)
Larheim, T., Abrahamsson, A., Kristensen, M., Arvidsson, L.: Temporomandibular joint diagnostics using cbct. Dentomaxillofacial Radiology44(1), 20140235 (2015)
2015
-
[14]
Journal of Den- tistry127, 104345 (2022)
Li, M., Punithakumar, K., Major, P.W., Le, L.H., Nguyen, K.C.T., Pacheco- Pereira, C., Kaipatur, N.R., Nebbe, B., Jaremko, J.L., Almeida, F.T.: Temporo- mandibular joint segmentation in mri images using deep learning. Journal of Den- tistry127, 104345 (2022)
2022
-
[15]
Li, Y., Wu, Y., Lai, Y., Hu, M., Yang, X.: Meddinov3: How to adapt vision foun- dation models for medical image segmentation? arXiv preprint arXiv:2509.02379 (2025)
arXiv 2025
-
[16]
Nature Communications15, 654 (2024)
Ma, J., He, Y., Li, F., Han, L., You, C., Wang, B.: Segment anything in medical images. Nature Communications15, 654 (2024)
2024
-
[17]
Dentomaxillofacial Radiology51(1), 20210185 (2022)
Nozawa, M., Ito, H., Ariji, Y., Fukuda, M., Igarashi, C., Nishiyama, M., Ogi, N., Katsumata, A., Kobayashi, K., Ariji, E.: Automatic segmentation of the tem- poromandibular joint disc on magnetic resonance images using a deep learning technique. Dentomaxillofacial Radiology51(1), 20210185 (2022)
2022
-
[18]
El- sevier Health Sciences (2019)
Okeson, J.P.: Management of Temporomandibular Disorders and Occlusion-E- Book: Management of Temporomandibular Disorders and Occlusion-E-Book. El- sevier Health Sciences (2019)
2019
-
[19]
In: AAAI
Perez, E., Strub, F., De Vries, H., Dumoulin, V., Courville, A.: Film: Visual rea- soning with a general conditioning layer. In: AAAI. vol. 32 (2018)
2018
-
[20]
Journal of applied oral science27, e20180433 (2019)
Poluha, R.L., Canales, G.D.l.T., Costa, Y.M., Grossmann, E., Bonjardim, L.R., Conti, P.C.R.: Temporomandibular joint disc displacement with reduction: a re- view of mechanisms and clinical presentation. Journal of applied oral science27, e20180433 (2019)
2019
-
[21]
In: MICCAI
Ronneberger, O., Fischer, P., Brox, T.: U-net: Convolutional networks for biomed- ical image segmentation. In: MICCAI. pp. 234–241. Springer (2015)
2015
-
[22]
Sato, S., Sakamoto, M., Kawamura, H., Motegi, K.: Long-term changes in clinical signsandsymptomsanddiscpositionandmorphologyinpatientswithnonreducing discdisplacementinthetemporomandibularjoint.Journaloforaland maxillofacial surgery57(1), 23–29 (1999)
1999
-
[23]
Journal of oral & facial pain and headache28(1), 6 (2014)
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J.P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., et al.: Diagnostic criteria for temporomandibular disorders (dc/tmd) for clinical and research applications: rec- ommendations of the international rdc/tmd consortium network and orofacial pain special interest group. Journal...
2014
-
[24]
In: CVPR
Shit, S., Paetzold, J.C., Sekuboyina, A., Ezhov, I., Unger, A., Zhylka, A., Pluim, J.P., Bauer, U., Menze, B.H.: cldice-a novel topology-preserving loss function for tubular structure segmentation. In: CVPR. pp. 16560–16569 (2021)
2021
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.