Recognition: unknown
PSIRNet: Deep Learning-based Free-breathing Rapid Acquisition Late Enhancement Imaging
Pith reviewed 2026-05-10 16:48 UTC · model grok-4.3
The pith
A deep learning network produces diagnostic-quality cardiac MRI images from a single two-heartbeat acquisition.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
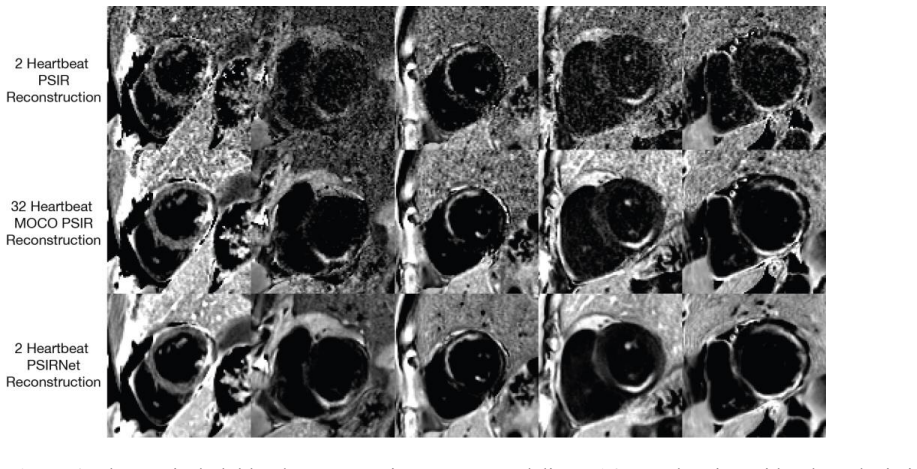
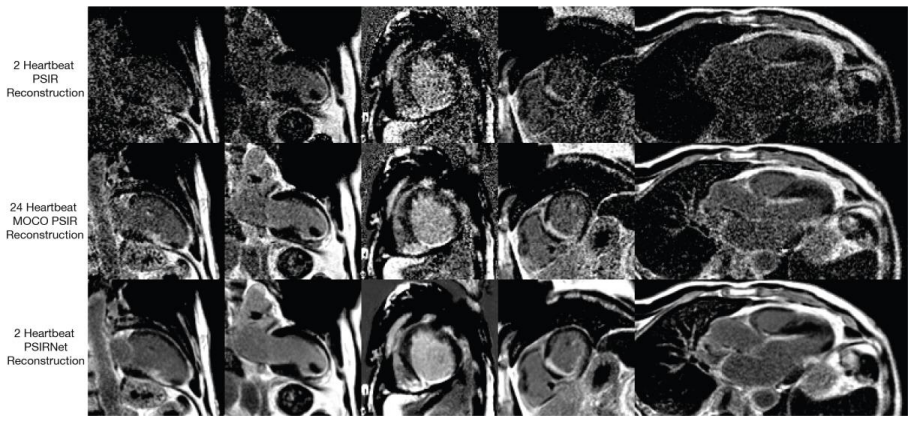
PSIRNet is a physics-guided deep learning network with 845 million parameters that reconstructs surface-coil-corrected PSIR images from a single interleaved IR/PD acquisition over two heartbeats. On held-out data from different institutions, single-average PSIRNet reconstructions received expert Likert scores superior to or equivalent with the reference MOCO PSIR images built from many averages, while taking roughly 100 ms per slice to compute versus more than 5 seconds.
What carries the argument
PSIRNet, a physics-guided deep learning network trained end-to-end to map single-acquisition k-space data to PSIR LGE images with surface coil correction.
If this is right
- Reduces acquisition time for free-breathing PSIR LGE by a factor of 8 to 24.
- Produces images at approximately 100 ms per slice instead of more than 5 seconds.
- Delivers quality rated superior for dark blood LGE and equivalent or superior for bright blood and wideband variants.
- Operates on data from both 1.5T and 3T scanners across multiple institutions.
Where Pith is reading between the lines
- Similar networks could shorten other cardiac MRI protocols that currently depend on extensive averaging for motion robustness.
- Clinical deployment might raise daily patient throughput in cardiac imaging suites.
- The multi-year multi-site training set suggests robustness, yet performance on post-2024 scanner hardware would need separate checks.
- The approach could support protocols for patients unable to perform repeated breath-holds.
Load-bearing premise
A model trained on retrospective multi-site data from 2016-2024 will continue to match or exceed standard image quality on new patients and scanners without retraining.
What would settle it
A prospective study collecting paired single-average and multi-average data on previously unseen patients and scanners, then showing expert ratings of PSIRNet images fall below equivalence margin on the 5-point Likert scale.
Figures



read the original abstract
Purpose: To develop and evaluate a deep learning (DL) method for free-breathing phase-sensitive inversion recovery (PSIR) late gadolinium enhancement (LGE) cardiac MRI that produces diagnostic-quality images from a single acquisition over two heartbeats, eliminating the need for 8 to 24 motion-corrected (MOCO) signal averages. Materials and Methods: Raw data comprising 800,653 slices from 55,917 patients, acquired on 1.5T and 3T scanners across multiple sites from 2016 to 2024, were used in this retrospective study. Data were split by patient: 640,000 slices (42,822 patients) for training and the remainder for validation and testing, without overlap. The training and testing data were from different institutions. PSIRNet, a physics-guided DL network with 845 million parameters, was trained end-to-end to reconstruct PSIR images with surface coil correction from a single interleaved IR/PD acquisition over two heartbeats. Reconstruction quality was evaluated using SSIM, PSNR, and NRMSE against MOCO PSIR references. Two expert cardiologists performed an independent qualitative assessment, scoring image quality on a 5-point Likert scale across bright blood, dark blood, and wideband LGE variants. Paired superiority and equivalence (margin = 0.25 Likert points) were tested using exact Wilcoxon signed-rank tests at a significance level of 0.05 using R version 4.5.2. Results: Both readers rated single-average PSIRNet reconstructions superior to MOCO PSIR for dark blood LGE (conservative P = .002); for bright blood and wideband, one reader rated it superior and the other confirmed equivalence (all P < .001). Inference required approximately 100 msec per slice versus more than 5 sec for MOCO PSIR. Conclusion: PSIRNet produces diagnostic-quality free-breathing PSIR LGE images from a single acquisition, enabling 8- to 24-fold reduction in acquisition time.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper claims to develop PSIRNet, a physics-guided deep learning network with 845 million parameters, that reconstructs diagnostic-quality phase-sensitive inversion recovery (PSIR) late gadolinium enhancement (LGE) cardiac MRI images from a single free-breathing interleaved IR/PD acquisition over two heartbeats. Trained end-to-end on a large retrospective multi-site dataset of 800,653 slices from 55,917 patients (2016-2024), with patient-wise splits and different institutions for train/test, it is evaluated against MOCO-averaged references using SSIM, PSNR, NRMSE and independent expert 5-point Likert scoring with Wilcoxon signed-rank tests for superiority and equivalence (margin 0.25), showing superiority or equivalence while reducing acquisition time by 8- to 24-fold.
Significance. If the retrospective performance generalizes, the work has high clinical significance by enabling much shorter free-breathing PSIR LGE scans without loss of diagnostic quality, which would improve throughput and patient tolerance in cardiac MRI. The large-scale multi-institutional patient-split dataset, quantitative metrics, and statistically tested expert ratings provide solid support for the performance claim on the evaluated distribution.
major comments (1)
- [Materials and Methods] Materials and Methods: The training and test data are drawn from the same 2016-2024 multi-institutional retrospective distribution (different institutions but no temporal hold-out after 2024 or scanners absent from training). With an 845-million-parameter model, this leaves untested the generalization to prospective acquisitions on new patients or hardware, which is load-bearing for the Conclusion claim that PSIRNet enables routine 8- to 24-fold acquisition-time reduction in clinical practice.
minor comments (2)
- [Results] Results: The Likert-scale superiority/equivalence findings are reported with p-values but without explicit mean/median values or confidence intervals per reader and variant; adding these would strengthen interpretability of the clinical equivalence margin.
- The inference-time comparison (~100 ms vs >5 s) is useful but lacks hardware specifications or details on whether MOCO time includes all post-processing steps.
Simulated Author's Rebuttal
We thank the referee for the constructive review and recommendation for minor revision. We address the single major comment below.
read point-by-point responses
-
Referee: [Materials and Methods] Materials and Methods: The training and test data are drawn from the same 2016-2024 multi-institutional retrospective distribution (different institutions but no temporal hold-out after 2024 or scanners absent from training). With an 845-million-parameter model, this leaves untested the generalization to prospective acquisitions on new patients or hardware, which is load-bearing for the Conclusion claim that PSIRNet enables routine 8- to 24-fold acquisition-time reduction in clinical practice.
Authors: We agree that the absence of prospective data on new patients and hardware constitutes a genuine limitation for claims of routine clinical deployment. The study is explicitly retrospective, with patient-wise splits and training/testing data drawn from different institutions to reduce data leakage. The dataset spans eight years, multiple sites, and both 1.5 T and 3 T field strengths, providing substantial diversity within the observed distribution. We will add an explicit limitations paragraph in the Discussion acknowledging the retrospective design and the requirement for prospective validation on unseen hardware and acquisition conditions. We will also revise the Conclusion to state that the method demonstrates diagnostic-quality reconstruction with the potential to enable 8- to 24-fold acceleration, subject to confirmation in prospective studies. revision: yes
Circularity Check
No significant circularity in derivation chain
full rationale
The paper presents an empirical deep-learning reconstruction method trained end-to-end on a large retrospective multi-site dataset (patient-wise split, different institutions for train/test) to map single-acquisition raw data to PSIR images. Quality is assessed on held-out test data via SSIM/PSNR/NRMSE against independent MOCO references and expert Likert scoring with statistical tests. No equations, ansatzes, or derivations are shown that reduce the claimed output to a fitted parameter, self-referential quantity, or self-citation chain by construction. The central result is an empirical performance comparison on independent data rather than any self-definitional or fitted-input-called-prediction pattern.
Axiom & Free-Parameter Ledger
free parameters (1)
- 845 million network parameters
axioms (1)
- domain assumption A physics-guided convolutional network can learn an accurate mapping from single-acquisition raw k-space to motion-corrected PSIR images
Reference graph
Works this paper leans on
-
[1]
Cardiac imaging techniques for physicians: late enhancement
Kellman P, Arai AE. Cardiac imaging techniques for physicians: late enhancement. J Magn Reson Imaging. 2012;36(3):529-542. doi:10.1002/jmri.23605
-
[2]
Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002;47(2):372-383. doi:10.1002/mrm.10051
-
[3]
Ledesma-Carbayo MJ, Kellman P, Hsu LY, Arai AE, McVeigh ER. Motion corrected free-breathing delayed-enhancement imaging of myocardial infarction using nonrigid registration. J Magn Reson Imaging. 2007;26(1):184-190. doi:10.1002/jmri.20957
-
[4]
Free-breathing late enhancement imaging: phase sensitive inversion recovery (PSIR) with respiratory motion corrected (MOCO) averaging
Kellman P, Xue H, Hansen MS. Free-breathing late enhancement imaging: phase sensitive inversion recovery (PSIR) with respiratory motion corrected (MOCO) averaging. MAGNETOM Flash. 2016;66:65–73
2016
-
[5]
El-Rewaidy H, Neisius U, Mancio J, et al. Deep complex convolutional network for fast reconstruction of 3D late gadolinium enhancement cardiac MRI. NMR Biomed. 2020;33(7):e4312. doi:10.1002/nbm.4312
-
[6]
van der Velde N, Hassing HC, Bakker BJ, et al. Improvement of late gadolinium enhancement image quality using a deep learning-based reconstruction algorithm and its influence on myocardial scar quantification. Eur Radiol. 2021;31(6):3846-3855. doi:10.1007/s00330-020-07461-w
-
[7]
Muscogiuri G, Martini C, Gatti M, et al. Feasibility of late gadolinium enhancement (LGE) in ischemic cardiomyopathy using 2D-multisegment LGE combined with artificial intelligence reconstruction deep learning noise reduction algorithm. Int J Cardiol. 2021;343:164-170. doi:10.1016/j.ijcard.2021.09.012
-
[8]
URL https://arxiv.org/abs/2102.09542
Yaman B, Shenoy C, Deng Z, Moeller S, El-Rewaidy H, Nezafat R, Akçakaya M. Self-supervised physics-guided deep learning reconstruction for high-resolution 3D LGE CMR. In: 2021 IEEE 18th International Symposium on Biomedical Imaging (ISBI). IEEE; 2021:100–104. doi:10.1109/ISBI48211.2021.9434054
-
[9]
Demirel OB, Ghanbari F, Hoeger CW, et al. Late gadolinium enhancement cardiovascular magnetic resonance with generative artificial intelligence. J Cardiovasc Magn Reson. 2025;27(1):101127. doi:10.1016/j.jocmr.2024.101127
-
[10]
Dark blood late enhancement imaging
Kellman P, Xue H, Olivieri LJ, et al. Dark blood late enhancement imaging. J Cardiovasc Magn Reson. 2016;18(1):77. Published 2016 Nov 7. doi:10.1186/s12968-016-0297-3
-
[11]
Bhuva AN, Kellman P, Graham A, et al. Clinical impact of cardiovascular magnetic resonance with optimized myocardial scar detection in patients with cardiac implantable devices. Int J Cardiol. 2019;279:72-78. doi:10.1016/j.ijcard.2019.01.005
-
[12]
Tyger v0.13.5
Microsoft. Tyger v0.13.5. Updated September 25, 2025. Accessed March 7, 2026. https://github.com/microsoft/tyger/releases/tag/v0.13.5
2025
-
[13]
Gadgetron: an open source framework for medical image reconstruction
Hansen MS, Sørensen TS. Gadgetron: an open source framework for medical image reconstruction. Magn Reson Med. 2013;69(6):1768-1776. doi:10.1002/mrm.24389
-
[14]
An iteration formula for Fredholm integral equations of the first kind
Landweber L. An iteration formula for Fredholm integral equations of the first kind. Am J Math. 1951;73(3):615-624
1951
-
[15]
Learning a variational network for reconstruction of accelerated MRI data
Hammernik K, Klatzer T, Kobler E, Recht MP, Sodickson DK, Pock T, Knoll F. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med. 2018;79(6):3055- 3071
2018
-
[16]
End-to-end variational networks for accelerated MRI reconstruction
Sriram A, Zbontar J, Murrell T, et al. End-to-end variational networks for accelerated MRI reconstruction. In: Medical Image Computing and Computer Assisted Intervention – MICCAI 2020. Springer; 2020:64-73. doi:10.1007/978-3-030-59713-9_7
-
[17]
In: Medical Image Compu ting and Computer-Assisted Intervention – MICCAI 2015
Ronneberger O, Fischer P, Brox T. U-Net: convolutional networks for biomedical image segmentation. In: Medical Image Computing and Computer-Assisted Intervention – MICCAI 2015. Springer; 2015:234-241. doi:10.1007/978-3-319-24574-4_28
-
[18]
Ulyanov D, Vedaldi A, Lempitsky V. Improved texture networks: Maximizing quality and diversity in feed-forward stylization and texture synthesis. In: 2017 IEEE Conference on Computer Vision and Pattern Recognition. IEEE; 2017:6924-6932. doi:10.1109/CVPR.2017.437
-
[19]
Rectifier nonlinearities improve neural network acoustic models
Maas AL, Hannun AY, Ng AY. Rectifier nonlinearities improve neural network acoustic models. In: Proceedings of the 30th International Conference on Machine Learning. 2013;30(1):3
2013
-
[20]
InProceedings of the IEEE/CVF conference on computer vision and pattern recognition
Wang Z, Bovik AC, Sheikh HR, Simoncelli EP. Image quality assessment: from error visibility to structural similarity. IEEE Trans Image Process. 2004;13(4):600-612. doi:10.1109/TIP.2003.819861
-
[21]
PyTorch: an imperative style, high-performance deep learning library
Paszke A, Gross S, Massa F, et al. PyTorch: an imperative style, high-performance deep learning library. Adv Neural Inf Process Syst. 2019;32:8024-8035
2019
-
[22]
Decoupled weight decay regularization
Loshchilov I, Hutter F. Decoupled weight decay regularization. In: Proceedings of the 7th International Conference on Learning Representations. 2019
2019
-
[23]
Confidence intervals based on bootstrap percentiles
Efron B, Tibshirani RJ. Confidence intervals based on bootstrap percentiles. In: An Introduction to the Bootstrap. Chapman and Hall/CRC; 1994:168-177
1994
-
[24]
Biometrics Bulletin , author =
Wilcoxon F. Individual comparisons by ranking methods. Biometrics Bull. 1945;1(6):80-83. doi:10.2307/3001968
-
[25]
A comparison of the two one-sided tests procedure and the power approach for assessing the equivalence of average bioavailability
Schuirmann DJ. A comparison of the two one-sided tests procedure and the power approach for assessing the equivalence of average bioavailability. J Pharmacokinet Biopharm. 1987;15(6):657-
1987
-
[26]
doi:10.1007/BF01068419
-
[27]
Remarks on zeros and ties in the Wilcoxon signed rank procedures
Pratt JW. Remarks on zeros and ties in the Wilcoxon signed rank procedures. J Am Stat Assoc. 1959;54(287):655-667. doi:10.1080/01621459.1959.10501526
-
[28]
A simple sequentially rejective multiple test procedure
Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6(2):65-70. doi:10.2307/4615733
-
[29]
R: A Language and Environment for Statistical Computing
R Core Team. R: A Language and Environment for Statistical Computing. Version 4.5.2. R Foundation for Statistical Computing. Updated October 31, 2025. Accessed March 7, 2026. https://www.r-project.org
2025
-
[30]
Statistical Hypothesis Testing in Context: Reproducibility, Inference, and Science
Fay MP, Brittain EH. Statistical Hypothesis Testing in Context: Reproducibility, Inference, and Science. Cambridge University Press; 2022
2022
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.